
Translate this page into:
Comparison of retention of two proximal sealants in mandibular first molars of 12-year-old school children - A split-mouth randomized trial
-
Received: ,
Accepted: ,
Abstract
Aim:
This study was done to assess and compare the retention properties of a proximal sealant made of polyurethane dimethacrylate and a resin-based adhesive system for sealing proximal surfaces of permanent mandibular first molars in 12-year-old children over a period of 6 months.
Methodology:
A split-mouth randomized trial was conducted among 50 school children. Pre-operative and post-operative bitewing radiographs were taken bilaterally prior at baseline and the end of the sixth month. Separators were placed for those children who did not have physiological spacing. The interventions were delivered on the left and right sides after randomization as per the manufacturer’s instructions, and post-operative instructions were given to the participants. The interventions were assessed for retention primarily and other criteria such as color match, marginal discoloration, marginal adaptation, anatomic form, caries formation (using bitewing radiographs), post-operative sensitivity, and surface roughness at the end of the 1st, 3rd, and 6 months using United States Public Health Service Modified Ryge Criteria for Direct Clinical Evaluation of Restorations proposed by Cvar and Ryge, 1980. The data were compiled, analyzed using SPSS and results were generated.
Conclusions:
The study results revealed that the resin-based adhesive system was better than the adhesive patch in terms of retention over a period of 6 months. Hence, the feasibility of including proximal sealants as a part of the preventive regimen for caries risk children should be positively considered.
Keywords
Dental caries
Permanent molars
Proximal surfaces
Resins
Sealants


INTRODUCTION
The World Health Organization has considered dental caries and periodontal disease to be two of the most important global health burdens due to the high worldwide prevalence of both conditions.[1] Dental caries is widespread, affecting 60–90% of school-age children and the majority of adults.[2] Although it is generally perceived that dental caries prevalence is reducing worldwide, there exists an opposing trend in caries prevalence among the industrialized countries which show a steady decline and an increase in the caries prevalence in developing nations, most likely due to the growing consumption of sugars and low exposure to fluoride.[3] In India, dental caries affects around 60% of the population.[4] The Ministry of Health and Family Welfare, GOI, accepted National Oral health policy as a component of National Health Programme and put forth a ten-point resolution in 1995 in which providing preventive and promotive oral health services in villages was introduced.[5] Placing pit and fissure sealants in school children was a part of this program. This was again emphasized in the draft of Oral Health Policy formulated in 2014 wherein application of proximal sealants for school children is advocated using private-public partnership model.[6] Epidemiological data suggest that dental caries in the permanent molars is a major issue in school children and it is suggested that up to 20% of these were initiated during the eruption period. Data also suggest that the proximal surfaces are more susceptible to caries in older children and young adults. At the age of 13 years, proximal caries constitutes approximately 30% of the annual caries increment, and it increases to about 50% at 27 years of age, respectively.[7] Hence, it is mandatory to take measures to detect these lesions in their initial stages, to avoid their progression, by means of preventive therapies and therefore preventing restorative treatment. Hence, during the formulation of an oral health preventive program, emphasis should be placed on sealing the proximal surfaces along with the occlusal surfaces of caries susceptible teeth. However, there is a scarcity of literature in Indian scenario regarding the retentive properties of these proximal sealants. Hence, this study was contemplated with the aim to evaluate and compare the retentive properties of two of these newer materials, a proximal sealant made of polyurethane dimethacrylate and an adhesive system made of alkyl dimethyl resins, placed on mandibular permanent first molars among 12-year-old subjects over a period of 6 months. The research hypothesis for the present study was there is a difference in the retention properties of proximal sealant made of polyurethane dimethacrylate and a resin-based adhesive system placed on mandibular permanent first molars among 12-year-old school children over a period of 6 months.
METHODOLOGY
This study design was a split-mouth randomized trial in a school-based field setting, done on 12-year-old school children in Chennai. Ethical clearance for this study was obtained by the Institutional Review Board of Ragas Dental College and Hospital, and this study was registered in clinical trials registry of India (REF/2015/07/009281). Permission was obtained from the school authorities, and parents’ consent was obtained in both the regional language (Tamil) and English. Children aged 12 years with fully erupted mandibular permanent first molars bilaterally and children scoring 1 according to the International Caries Detection and Assessment System II[8] criteria for recording proximal caries in the mesial surface of their mandibular permanent first molars, bilaterally and children not suffering from any apparent systemic illness/disease were included in the study. Children who had enamel defects such as amelogenesis imperfecta, enamel hypoplasia, and dental fluorosis, children suffering from any acute dental infection and children who underwent orthodontic treatment were excluded from the study. This study was done using a split-mouth design, and hence, interventions were placed on the mesial surfaces of the right and left mandibular molars of the subject randomly. A single calibrated investigator placed all the interventions and recorded all criteria based on the United States Public Health Service - Modified Ryge Criteria for Direct Clinical Evaluation of Restorations[9] criteria for all the sealants and patches.
Sample size estimation: The sample size for each group was calculated using the PharmaSchool Sample Size calculator for clinical trials[10] (software to calculate the sample size for equivalence trials). After the necessary input values, the sample size estimated was 34 in each group. Hence, anticipating drop out of subjects in the follow-up period, the sample size was increased by 10% that is 50 for each intervention. Since the study design was a split-mouth study, 50 subjects were chosen to deliver a total of 100 interventions, 50 on each side.
A total of 600, 12-year-old (age at the last birthday and those belonging to Class VI and Class VII) children were screened at the school premises. All 600 students were screened using Type III oral examination as recommended by the American Dental Association. Finally, a total of 68 subjects, who met the inclusion criteria were identified after which, a total of 50 subjects who consented for this study were included for the study.
At the start of the study, bitewing radiographs of the mandibular first permanent molars were taken bilaterally using the portable radiograph unit (ProX wireless portable X-ray, DigiMed, Korea) and bitewing radiograph films (e-speed dental films, Carestream) which were developed using portable radiograph developing unit.
Randomization was done in allocating the right and left sides for the interventions using coin toss method.
Description of the Interventions
-
Intervention A: Proximal sealant[11] made of polyurethane dimethacrylate tape marketed as Tegaderm®, 3M company, manufactured at Germany and imported to India.
-
Intervention B: A resin-based adhesive system[12] made of alkyl dimethyl resin marketed as Optibond S®, a two-step etch and rinse adhesive system marketed by Kerr, Orange, CA, and USA.
After randomization, separators were placed[13] (only for those children who did have normal physiological spacing) between the mandibular second premolar and mandibular first molar for a period of 24–48 h after which the interventions were placed as per the manufacturer’s instructions[11,12]. The clinical procedure was carried out on each subject by placement of one of the interventions on the right molar on the 1st day, and the other intervention was placed on the left side on a subsequent day. A total of 100 interventions, 2 for each patient, on the left and right side was placed. It took 10 days to complete this procedure with 10 interventions placed on each day and the time taken to place each intervention was around 20 min. The subjects were asked not to rinse their mouth for 30 min and consume any food substance for about 1 h after placing the interventions.
Assessment of Outcome Variables
Clinical assessments were made at the end of 1st month, 3rd month, and 6th month in the school premises. No dropouts were noted. Primarily, the retention of the interventions was assessed. Along with it, the other factors such as color match, marginal discoloration, secondary caries, anatomic form, marginal adaptation, post-operative sensitivity, and surface texture were also assessed. Endodontic loupes were used additionally, to confirm the presence or absence of the patch. At the end of each follow-up, the subjects were asked if they had any discomfort in the approximal surfaces of the sealed teeth during the study period and were rectified. At the end of the 6th month, post-operative bitewing radiographs were taken bilaterally to assess if there was caries progression after the placement of the interventions [Chart 1].
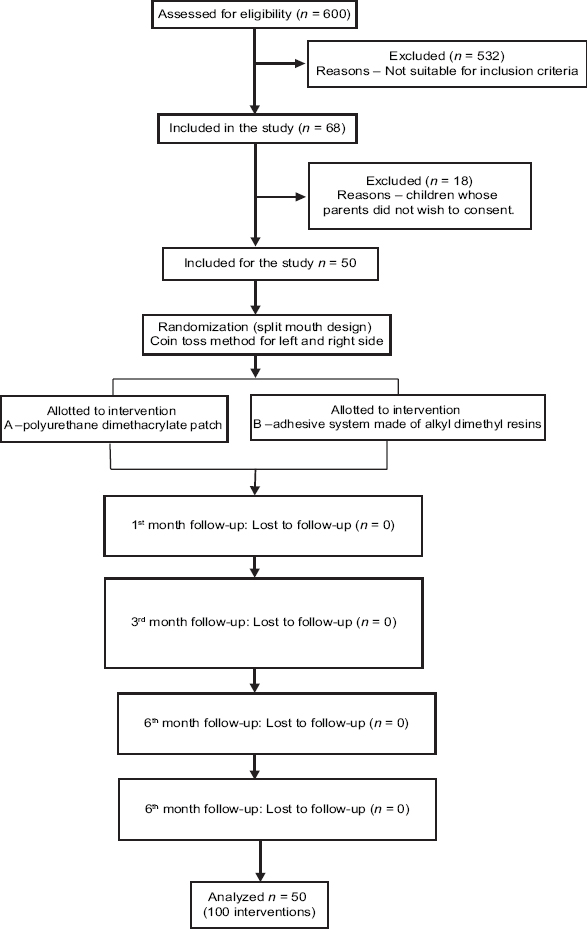
- Flowchart illustrating the methodology of the study.
Statistical Analyses
Statistical analyses were performed in the Statistical Package for the Social Sciences software (SPSS version 19, USA). P value of <0.05 (P < 0.05) was considered to be significant. Chi-square test was used to analyze all the qualitative data, intergroup and intragroup comparisons at the end of 1st, 3rd, and 6th months.
RESULTS
A total of 24 males and 26 females participated in the study. There were no dropouts throughout the study period. Hence, analysis was done for all the 100 interventions placed. The primary outcome retention was analyzed along with the outcomes such as color match, marginal discoloration, secondary caries, anatomic form, marginal adaptation, post-operative sensitivity, and surface texture.
Retention
Table 1 shows the distribution based on retention of the interventions at the end of the 1st, 3rd, and 6th months. The difference in the retention between the interventions was statistically significant at the end of 6 months (P = 0.026). The line diagram [Figure 1] shows the comparison of retained interventions at the end of the 1st, 3rd, and the 6th months.
| Scoring criteria | 1st month | 3rd month | 6th month | |||
|---|---|---|---|---|---|---|
| Intervention A | Intervention B | Intervention A | Intervention B | Intervention A | Intervention B | |
| Retained | 45 | 48 | 35 | 44 | 30 | 42 |
| Partially retained | 4 | 1 | 13 | 5 | 14 | 5 |
| Missing | 1 | 1 | 2 | 1 | 6 | 3 |
| P value | 0.387 | 0.086 | 0.026 | |||
| Chi-square value | 1.897 | 4.414 | 7.263 | |||

- Distribution based on retained interventions (Score A) between the interventions at 1, 3, and 6 months.
Other Criterion
Table 2 shows the distribution based on a comparison of other outcomes such as color match, marginal discoloration, marginal adaptation, caries formation, post-operative sensitivity, and surface texture. The results were dichotomized into clinically acceptable (Score A and B) and clinically unacceptable (Score C) for easy representation of results in case of other criteria. Comparison of all the other criteria such as color match, marginal discoloration, marginal adaptation, anatomic form, post-operative sensitivity, and surface roughness between both the interventions was not statistically significant during all the follow-ups (1st, 3rd, and 6th months) (P > 0.05) [Table 2].
| Parameter | Time point | Scoring criteria | Interventions | Chi-square value | P value | |
|---|---|---|---|---|---|---|
| Intervention A | Intervention B | |||||
| Color match | 1st month | Acceptable | 47 | 42 | 3.059 | 0.080 |
| Not acceptable | 2 | 7 | ||||
| 3rd month | Acceptable | 40 | 33 | 3.328 | 0.055 | |
| Not Acceptable | 8 | 16 | ||||
| 6th month | Acceptable | 34 | 29 | 2.586 | 0.083 | |
| Not acceptable | 10 | 18 | ||||
| Marginal discoloration | 1st month | No discoloration | 47 | 43 | 2.174 | 0.134 |
| Staining present | 2 | 6 | ||||
| 3rd month | No discoloration | 42 | 43 | 0.114 | 0.484 | |
| Staining present | 6 | 6 | ||||
| 6th month | No discoloration | 34 | 39 | 0.466 | 0.337 | |
| Staining present | 10 | 8 | ||||
| Marginal adaptation | 1st month | Acceptable | 48 | 44 | 2.841 | 0.102 |
| Unacceptable | 1 | 5 | ||||
| 3rd month | Acceptable | 45 | 44 | 1.693 | 0.167 | |
| Unacceptable | 3 | 7 | ||||
| 6th month | Acceptable | 38 | 40 | 0.029 | 0.552 | |
| Unacceptable | 6 | 7 | ||||
| Caries formation | At the end of 6th month | No evidence of caries | 50 | 50 | – | – |
| Evidence of caries along the margin of the restoration | 0 | 0 | ||||
| Anatomic form | 1st month | Acceptable | 48 | 45 | 1.897 | 0.181 |
| Unacceptable | 1 | 4 | ||||
| 3rd month | Acceptable | 45 | 43 | 1.035 | 0.254 | |
| Unacceptable | 3 | 6 | ||||
| 6th month | Acceptable | 38 | 41 | 0.015 | 0.573 | |
| Unacceptable | 6 | 6 | ||||
| Post-operative sensitivity | 1st month | Absent | 50 | 47 | 3.073 | 0.079 |
| Present | 0 | 3 | ||||
| 3rd month | Absent | 47 | 48 | 0.211 | 0.646 | |
| Present | 3 | 2 | ||||
| 6th month | Absent | 45 | 45 | 0.000 | 1.000 | |
| Present | 5 | 5 | ||||
| Surface texture | 1st month | Smooth | 41 | 40 | 0.071 | 0.500 |
| Rough | 8 | 9 | ||||
| Missing | 1 | 1 | ||||
| 3rd month | Smooth | 33 | 33 | 0.022 | 0.528 | |
| Rough | 15 | 16 | ||||
| Missing | 2 | 1 | ||||
| 6th month | Smooth | 34 | 24 | 2.760 | 0.074 | |
| Rough | 14 | 23 | ||||
| Missing | 6 | 3 | ||||
Pre-operative (at the start of the study) and post-operative bitewing radiographs (at the end of 6 months) which were taken bilaterally to assess the caries formation after the placement of the interventions showed that there was no caries formation in any intervention after a period of 6 months [Table 2].
DISCUSSION
The adhesive patch used in this study is a methacrylic, urethane-based, and polymer material of approximately 100-μm thickness. A series of in vitro studies have proven that the modification of adding an adhesive patch offers good chemomechanical properties.[14,15] The elastic polyurethane foil allows an even layer of bonding/sealant under the patch, more controllable application, and the removal of excess cervical bonding before light curing. In addition, this adhesive patch approach seems to be statistically more resistant to lactic acid exposure than two layers of enamel bonding, which has been proved in vitro.[15] The continuous patch also provides excellent protection in a cariogenic environment.[14]
The major advantage of resin application is the higher efficiency in the removal of white-spot lesion comparing with other remineralization methods. The flow of resin can deeply penetrate demineralized enamel surface through capillarity and can restore enamel structure from depth to surface. Studies have been done earlier to prove the effectiveness and caries preventing potential of these proximal sealants.[11,16-22]
The results of the present study showed that retention of the resin-based adhesive system was better than the adhesive patch at the end of 6 months. This may be due to better penetrating effects of the resin into the enamel thereby promoting remineralization of the lesions, whereas the adhesive patch acts only as a mechanical barrier with the presence of the underlying bonding agent. At the end of 6 months, a total of 6 adhesive patches were lost completely. This may be due to the mechanical stress due to regular oral hygiene practices. Apart from the completely lost restorations, partially missing restorations were more in the case of adhesive patches. This might be worse than the completely missing patches as it would attract plaque. In the present study; however, all the children were given oral hygiene instructions individually to prevent plaque or food accumulation in the interdental spaces. Further, they were also monitored regularly for the progression of caries at the interproximal study area.
Similar studies conducted by Abuchaim et al., 2010, on 44 adolescents on showed that therapeutic sealing of the proximal surfaces using a resin-based adhesive system was better than the controls which were monitored using oral hygiene measures. There was a significant reduction in the caries progression and at the end of 2 years almost 83% of the interventions were retained and either showed regression of caries or no change,[11] and another study conducted by Alkilzy et al., 2009, on the feasibility of using polyurethane dimethacrylate patch, the results showed that among a total of 36 restorations, 19% were completely lost and 81% were retained at the end of 2 years. The reasons stated by the authors of the study were probably due to the mechanical stresses of the proximal flossing.[18] This finding was in line with our present study.
The present study showed there was no caries formation in any of the interventions. The bitewing radiographs showed no change at the end of 6 months. However, these results could be confounded by the shorter duration of this study.
The strengths of this study: Literature shows that studies have been done earlier individually to assess the caries prevention potential of these two proximal sealants; however, to the best of our knowledge, this was the first-ever study to compare the retention properties of these interventions. The present study was conducted among 12-year school children, as studies have shown that this is the right age for the delivery of proximal sealants due to the presence of physiological spacing. Further, in children where there was an absence of physiological spacing, an elastic separator was used to create space before the procedure was carried out. Rubber dam was used for all the patients, as it isolated the operating field from moisture and blood contamination. Further, it prevented excess bonding agent from entering the proximal gingival sulcus. It also helped to retract the gingiva and provided good overall view during this technique sensitive procedure. Endodontic loupes were used to assess the outcome variables for better assessment. Pre- and post-operative bitewing radiographs were taken to assess caries progression, even though the study duration was 6 months. This was to confirm that no deleterious or harmful effects were done to the enamel or tooth structure after placement of the interventions. Occlusal pit and fissure sealant were applied to those subjects who had deep pits and fissures before the start of the study ensuring a proper occlusal seal.
However, there were certain limitations in the study, the study duration for the present study was 6 months; however, efforts should be taken to follow-up for a period of 2 or 3 years for assessing longetivity and caries progression. The present study was conducted on a defined population; however, further studies are needed to extrapolate the study findings for generalizability.
CONCLUSIONS
The overall study results showed that the resin-based adhesive system was better than the polyurethane dimethacrylate adhesive patch in terms of retention at the end of 6 months. However, assessment of all the other outcome variables, such as color match, marginal discoloration, marginal adaptation, anatomic form, and surface roughness between both the interventions showed that there was no much difference. The outcome of this study would be useful for policy framers to include proximal sealants as an adjuvant preventive regimen for caries risk population.
Acknowledgments
Our sincere acknowledgments to all the parents, participants, school teachers, and the principal of the school for helping us complete this study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- The world oral health report. 2003: Continuous improvement of oral health in the 21st century the approach of the WHO global oral health programme. Community Dent Oral Epidemiol. 2003;31(Suppl 1):3-23.
- [Google Scholar]
- What is the Burden of Oral Disease?Oral Disease Burdens and Common Risk Factors. Available from: http://www.who.int/oral_health/disease_burden/global/en/index.html
- Oral and Dental Diseases: Causes, Prevention and Treatment Strategies. New Delhi, India: A Manual of Burden of Disease in India; 2005. p. :275-98.
- National oral health care programme (NOHCP) implementation strategies. Indian J Community Med. 2004;24:3-10.
- [Google Scholar]
- Assessment of the status of national oral health policy in India. Int J Health Policy Manag. 2015;4:575-81.
- [Google Scholar]
- Two compliance-free and site-specific caries control techniques: Prefissure and proximal sealants. Int Dent S Afr. 2012;2:38-42.
- [Google Scholar]
- International caries detection and assessment system (ICDAS): A New concept. Int J Clin Pediatr Dent. 2011;4:93-100.
- [Google Scholar]
- Reprint of criteria for the clinical evaluation of dental restorative materials. 1971. Clin Oral Investig. 2005;9:215-32.
- [Google Scholar]
- Practical guide to sample size calculations: Non-inferiority and equivalence trials. Pharm Stat. 2016;15:80-9.
- [Google Scholar]
- Effectiveness of sealing active proximal caries lesions with an adhesive system: 1-year clinical evaluation. Braz Oral Res. 2010;24:361-7.
- [Google Scholar]
- Penetration of three adhesives in proximal white spot carious lesions: An in vitro study. Rev Fac Odontol Univ Antioq. 2012;24:84-95.
- [Google Scholar]
- Orthodontics: The Art and Science (5th ed). New Delhi: Arya Medi Publishers; 2012.
- Caries-preventive potential of an adhesive patch after thermomechanical loading a microbial-based in vitro study. J Adhes Dent. 2006;8:7-12.
- [Google Scholar]
- Sealing smooth enamel surfaces with a newly devised adhesive patch: A radiochemical in vitro analysis. Dent Mater. 2005;21:545-50.
- [Google Scholar]
- Plastic sealing of proximal surfaces of teeth, a new technic. J Baltimore Coll Dent Surg. 1975;30:40-7.
- [Google Scholar]
- Infiltration of resin into white spot caries-like lesions of enamel: An in vitro study. Eur J Prosthodont Restor Dent. 2002;10:27-32.
- [Google Scholar]
- Sealing proximal surfaces with polyurethane tape: Three-year evaluation. Clin Oral Investig. 2011;15:879-84.
- [Google Scholar]
- A 2-year clinical evaluation of sealed noncavitated approximal posterior carious lesions in adolescents. Clin Oral Investig. 2005;9:239-43.
- [Google Scholar]
- Infiltrating/sealing proximal caries lesions: A 3-year randomized clinical trial. J Dent Res. 2012;91:288-92.
- [Google Scholar]
- Therapeutic seal of approximal incipient noncavitated carious lesions: Technique and case reports. Quintessence Int. 2007;38:e99-105.
- [Google Scholar]
- Sealing of proximal surfaces with polyurethane tape: A two-year clinical and radiographic feasibility study. J Adhes Dent. 2009;11:91-4.
- [Google Scholar]




