
Correcting posterior transverse inter-arch discrepancy with non-helical expander – A prospective study

*Corresponding author: Ragini Rajesh Ogale, Department of Orthodontics and Dentofacial Orthopaedics, Rural Dental College, Pravara Institutes of Medical Sciences, Loni, Maharashtra, India. raginiogale1907@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Toshniwal N, Nair S, Manerikar R, Ogale RR, Mishra S. Correcting posterior transverse inter-arch discrepancy with non-helical expander – A prospective study. J Global Oral Health. doi: 10.25259/JGOH_34_2024
Abstract
Introduction
Transverse maxillary deficiency and maxillary crowding in children are problems commonly encountered and treated by orthodontists. Early treatment with palatal expansion has been recommended for children with transverse discrepancies. Slow expansion is commonly accomplished with appliances such as the W-arch or the Quad Helix. As the concept of Non-Helical Appliance (NHA) is fairly recent, the functioning of the appliance has not been verified on a large population. Hence, an attempt has been made in the present study to evaluate the expansion effect in the early mixed dentition with the new NHA.
Materials and Methods
A prospective longitudinal study was conducted in a total of 15 patients. Samples were collected of the patients with mixed dentition having transverse maxillary deficiency, of both sexes reporting to the Department of Orthodontics and Dentofacial Orthopedics, Rural Dental College, Loni. Necessary diagnostic records were taken. The sample group was given the Non-Helical palatal expander. Follow-ups were at one and six months. Pre- and post-treatment study models and maxillary occlusal radiographs were evaluated and compared for the arch width and arch length changes.
Results
This study showed that, the non-helical palatal expander is significantly efficacious in causing maxillary expansion in relation to the variables used in this study.
Discussion
The inter-canine, inter-premolar, and inter-molar width changes showed that significant amount of expansion was caused by the Non-helical expander appliance, that was comfirmed on the study models as well as the occlusal radiographs.
Keywords
Class II malocclusion
Mixed dentition
Transverse discrepancy
Non-helical expander appliance
Expansion

INTRODUCTION
In the context of Class II malocclusion development among young individuals, the transverse dimension is frequently the most affected. Transverse malocclusion is prevalent in approximately 30% of the Indian population.[1] A constricted maxillary arch can restrict the development of the mandible, resulting in functional retrognathism or retrognathic positioning of the mandible. This constricted “V”-shaped maxillary arch leads to a reduction in both inter-canine and inter-molar widths. This leads to posterior cross-bite, increased overjet and overbite, proclination of maxillary incisors, deep palatal vault, increased overjet and overbite, V shape arch, convex profile, narrow arch, and incompetent lips.[2] To address the constriction of the maxillary arch, various modalities of palatal expansion have been introduced, which can be classified as either slow maxillary expansion (SME) or rapid maxillary expansion (RME). The assessment of palatal expansion varies and may include methods such as Pont’s analysis and the Posterior Transverse Inter-arch Discrepancy protocol. Palatal enlargement is indicated in several conditions, including posterior crossbite, arch-width discrepancies between the maxilla and the mandible, and the necessity to enlarge the airway.[3] Research indicates that the prevalence of posterior crossbite in children with primary and mixed dentitions – who do not present with craniofacial anomalies – ranges from 7.7% to 23.3%.[4-6] A posterior crossbite occurs when the maxillary dentition is more constricted than the mandibular dentition. Specifically, unilateral posterior crossbites cause a functional shift in the ‘2’ position of the mandible, which can lead to skeletal asymmetry, condylar changes, and dental compensation.[7] The Quad Helix (QH) appliance is the most frequently employed device for correcting posterior crossbite in mixed dentition. This appliance is constructed from circular stainless-steel wire, typically with diameters of 0.030 inches or 0.036 inches, and is characterized by increased flexibility and force endurance.[8] Notably, the appliance may induce molar tipping, inflammation, and lesions on the tongue, and it is not considered hygienic due to the potential entrapment of food particles within the helices.[9]
To mitigate these concerns, Dr. Gerald W. Spencer proposed “The non-helical appliance (NHA): An Alternative to the QH.” This appliance resembles that the QH yet is devoid of helices and is fabricated from 0.036-inch round beta-titanium wire. The lateral expansion arms of this appliance are specifically designed to conform to the lingual features of the dentition. The palatal section is rounded anteriorly and is shaped to align with the arch following appropriate adjustment of the lateral arms. This configuration allows for efficient “fan expansion” of a V-shaped arch, facilitating the correction of any mesial rotation of the upper first molar. The NHA is adaptable for bilateral expansion and distalization, as well as for applying distal forces to the contralateral molar. Furthermore, an anterior bite plane may be integrated to facilitate bite opening.[10] Given that the concept of the NHA as an alternative to the conventional QH is relatively novel, its efficacy has not been thoroughly validated, and there exists a paucity of literature comparing this new appliance with traditional alternatives. Consequently, the objective of this study is to evaluate the efficacy of non-helical palatal expanders in growing patients with transverse maxillary discrepancies, utilizing study models and occlusal radiographs for assessment.
MATERIALS AND METHODS
The randomized clinical trial was conducted within the Department of Orthodontics and Dentofacial Orthopedics at Rural Dental College, Loni. The objective of this research is to evaluate the efficacy of conventional helical palatal expanders in comparison to non-helical palatal expanders in growing patients exhibiting transverse maxillary discrepancies. The Institutional Ethical Committee has granted approval for the aims and objectives of this study (number# 142). The sample size included a total of 30 participants (15 individuals in each group). The sample size was calculated using the A.P. Kulkarni Excel spreadsheet software, ensuring a 90% confidence limit and an 80% power for the study. Participants were selected in accordance with established inclusion and exclusion criteria. Samples consisted of patients aged between 7 and 12 years of both genders, who were in the early mixed dentition stage. Eligible patients who consented to undergo treatment were assigned to groups using a random lottery method. The criteria for patient selection is as follows: The patients in early, intermediate, or late mixed dentition; patients in cervical vertebral maturation index (CVMI) stages 1-3; patients presenting with transverse maxillary discrepancies identified as unilateral or bilateral skeletal posterior crossbites; and patients whose parents or guardians provided written informed consent for participation in the study.
The NHA is constructed from 0.036” round beta titanium wire. The lateral expansion arms of the appliance are specifically designed to adapt to the lingual aspects of the dentition. The palatal portion is bent over the lateral arms and rounded anteriorly to conform to the contour of the arch, positioned just lingual to the anterior teeth. This V-shaped arch can be easily “fan-expanded” to rectify any mesial rotation of the upper first molars. Furthermore, the NHA can be adjusted to exert a distal force on the contralateral molar or facilitate bilateral expansion and distalization [Figures 1 and 2].[8]
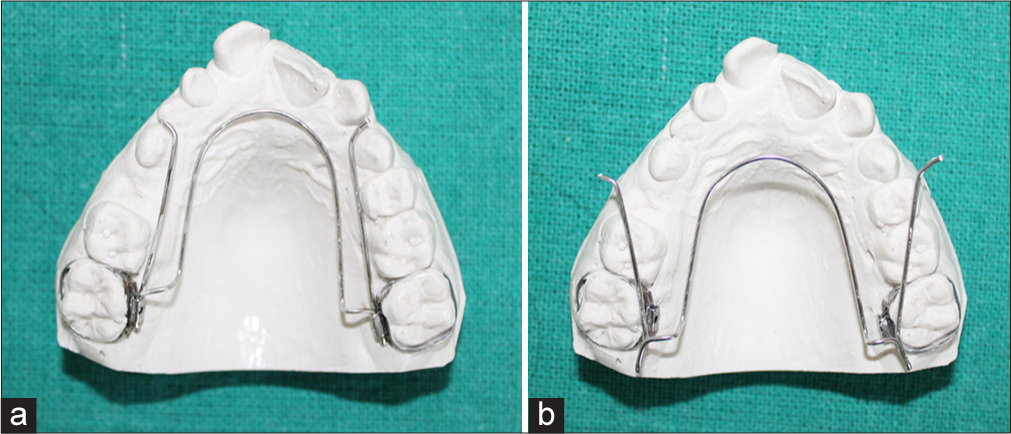
- Non-helical expander appliance with lateral in (a) active and (b) passive state.

- Intra-oral image of non-helical expander appliance with lateral arms activated.
In this study, essential and supplementary diagnostic tools were employed to assess both groups at the initial stage and after a 6-month protocol. Essential diagnostic aids included, (a) case history, (b) clinical examination, (c) study model impressions, (d) necessary radiographs, and (e) diagnostic photographs of the patients. Supplementary diagnostic aid included occlusal radiograph. Analysis of the study models was conducted to evaluate changes before and after treatment with NHAs in the following variables: (a) Arch widths at the canine, premolar, and molar regions; (b) Posterior transverse inter-arch discrepancy (the difference between maxillary and mandibular intermolar widths); (c) Tooth size-arch length discrepancy. The analysis of occlusal radiographs was performed to assess changes before and after the treatment with NHAs in terms of: (a) Arch widths in the canine, premolar, and molar areas, and (b) Mid-palatine suture ossification. All results were subjected to statistical analysis utilizing either the Student’s t-test or the paired Student’s t-test, depending on the relevant variables. Statistical significance was defined as highly significant at the 0.1% (P < 0.01) level, significant at the 5% (P < 0.05) level, and non-significant above the 5% (P > 0.05) level.
RESULTS
Table 1 shows comparison between pre- and post-treatment mean difference values of the change in the inter-canine, inter-premolar, and inter-molar width as well as the decrowding of anteriors, change in proclination, and the increase in the spacing seen in the study models for the experimental group that have been given the NHA [Figure 3]. There is a significant increase in the inter-canine, inter-premolar, and inter-molar widths after the treatment. The pre- and post-treatment mean difference values of the inter-canine width were 2.767 ± 0.4370, while that of inter-premolar widths was 2.320 ± 0.2426. Similarly, the pre- and post-treatment mean difference values of intermolar width were 3.893 ± 0.2685. Statistically, the increase in all the 3 widths was extremely significant.
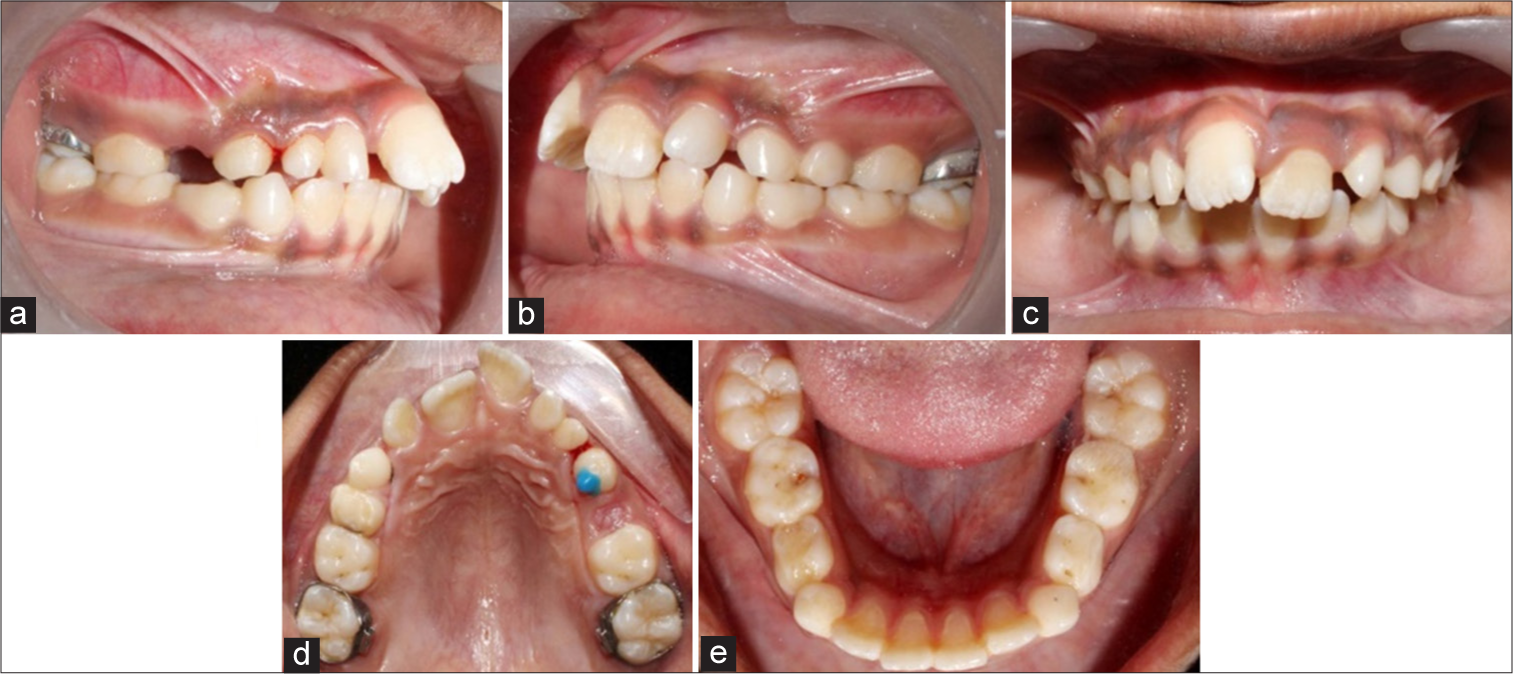
- (a-e) Post non-helical expander appliance treatment.
| Mean difference | SD difference | P-value | T-value | Degrees of confidence | Significance | |
|---|---|---|---|---|---|---|
| Intercanine width (mm) | 2.767 | 0.4370 | <0.0001 | 24.521 | 14 | Extremely significant |
| Inter premolar width (mm) | 2.320 | 0.2426 | <0.0001 | 37.037 | 14 | Extremely significant |
| Intermolar width (mm) | 3.893 | 0.2685 | <0.0001 | 56.158 | 14 | Extremely significant |
| Decrowding of anteriors | −0.3333 | 0.3086 | 0.0009 | 4.183 | 14 | Extremely significant |
| Proclination by direct method | −0.1333 | 0.2289 | 0.0406 | 2.256 | 14 | Significant |
| Spacing | 0.3333 | 0.3086 | 0.0009 | 4.183 | 14 | Extremely significant |
NHA: Non-helical appliance, SD: Standard deviation
The pre- and post-treatment mean difference values for decrowding of anteriors were −0.3333 ± 0.3086 while that for proclination by direct method decreased by −0.1333 ± 0.2289. The mean difference of the pre and post treatment values for the spacing was 0.3333 ± 0.3086. All the three values were statistically significant [Graph 1]. Table 1 also shows the T-value statistical analysis for the difference of the pre- and post-treatment values of the control group with extreme significance. Table 2 shows the comparison between pre- and post-treatment mean difference values seen on the occlusal radiograph of the change in the inter-canine, inter-premolar, and inter-molar width as well as the decrowding of anteriors, change in proclination, and the increase in the spacing for the experimental group that have been given the NHA. The pre- and post-treatment mean difference values of the inter-canine and inter-premolar widths were 1.760 ± 0.7249 and 1.613 ± 0.5668. Similarly, the pre- and post-treatment mean difference values of intermolar width were 5.267 ± 0.4952. Statistically, the increase in all the 3 widths was extremely significant. Table 2 also shows the T value statistical analysis for the difference of the pre- and post-treatment values of the control group with extreme significance [Graph 2].
| Mean difference | SD difference | P-value | T-value | Degrees of confidence | Significance | |
|---|---|---|---|---|---|---|
| Intercanine width (mm) | 1.760 | 0.7249 | <0.0001 | 9.404 | 14 | Extremely Significant |
| Inter Premolar width (mm) | 1.613 | 0.5668 | <0.0001 | 11.024 | 14 | Extremely Significant |
| Intermolar width (mm) | 5.267 | 0.4952 | <0.0001 | 19 | 14 | Extremely Significant |
NHA: Non-helical appliance, SD: Standard deviation
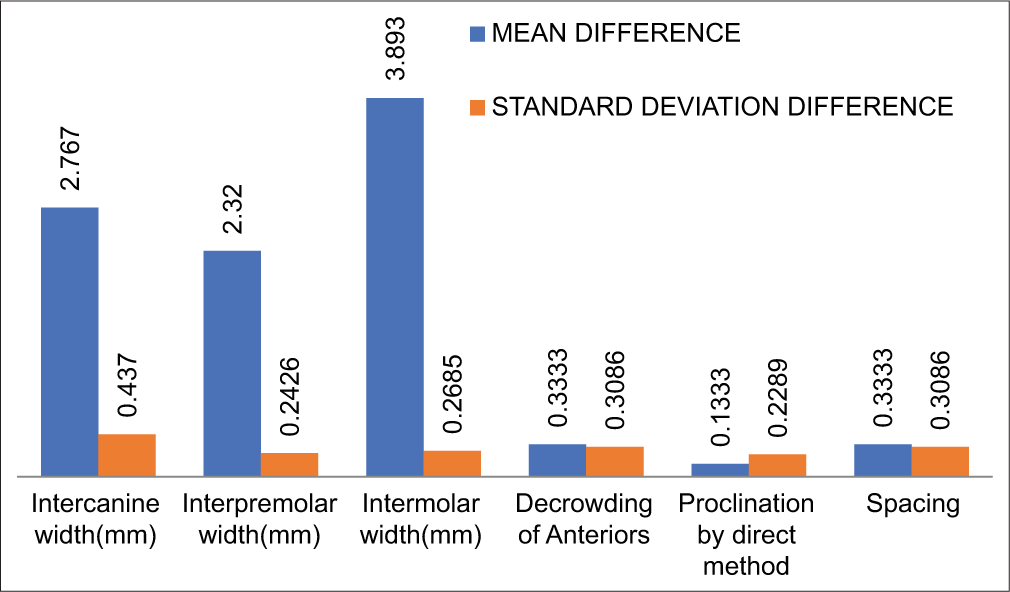
- Statistical analysis of evaluation of study models for pre and post-treatment of sample group with non-helical appliance.
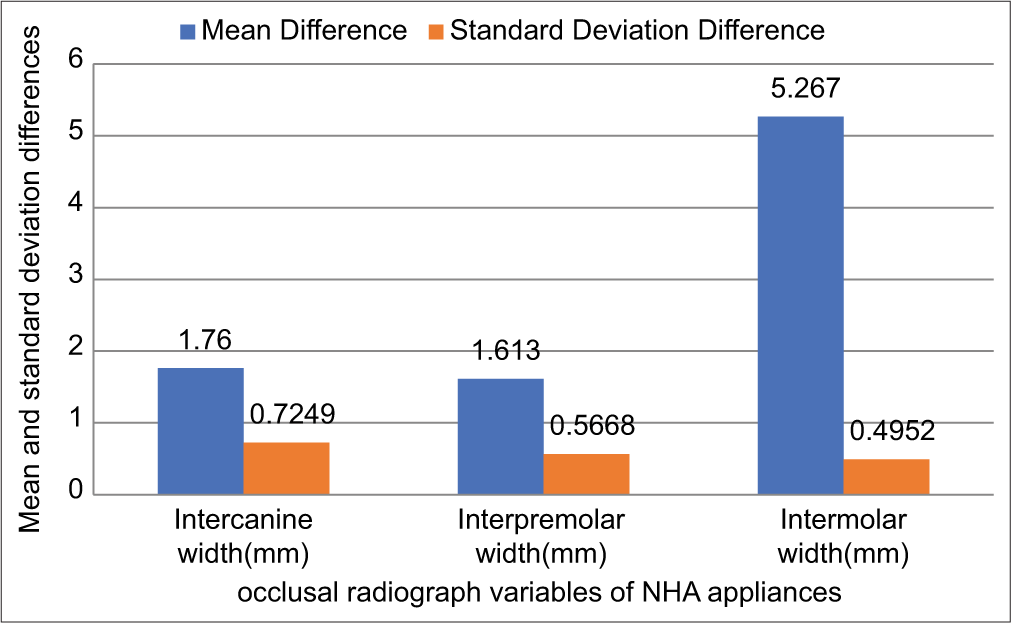
- Statistical analysis of evaluation of occlusal radiograph for pre- and post-treatment of sample group with non-helical appliance.
DISCUSSION
McNamara Jr. claims that transverse skeletal imbalances are often overlooked or not properly identified, resulting in fewer treatment options for individuals with these issues compared to those whose transverse skeletal imbalances are recognized. Among the regions of the craniofacial complex, the maxilla exhibits the most flexibility in its transverse dimension. During the deciduous and mixed dentition periods, posterior crossbite is one of the malocclusions that are most commonly observed. According to Kutin and Hawes,[8] the prevalence of this malocclusion is 8% in deciduous dentition, 12% in mixed dentition, and 7.2% in deciduous dentition, according to Kapoor et al.[1] Many researchers assert that this anomaly is not self-correcting and advise seeking treatment as soon as possible. Functional posterior cross-bites show a lateral shift of the mandible to avoid occlusal interferences. The mandibular shift produces a midline deviation, a unilateral cross-bite involving multiple teeth, and a condylar rotation toward the cross-bite side. Subsequent dental, skeletal, and neuromuscular adaptation results in a constricted maxillary arch of insufficient width to encompass the mandibular arch in a normal closure pattern.[11]
Maxillary expansion is a well-established treatment protocol for correcting maxillary transverse deficiency. The success of expansion is dependent on the patency of the mid-palatal suture There are two ways to achieve palatal expansion: RME and SME. Melsen found the mid-palatal suture fuses at age 16 years in females and 18 years in males.[12] The QH appliance, as described by Brandt and Ricketts in 1975,[12-15] is a modification of the earlier transpalatal coffin spring. It has four helical loops, each of which comprises an extra 25-mm wire which lightens the force magnitude. This helps in providing continuous action during expansion due to greater range of activation provided by the longer wire. A QH appliance is not only used for arch expansion but also can be activated to derotate the molar on one side of the arch, thus providing a distalizing force on the opposite side of the same arch. Thus, it is a multifunctional multipurpose appliance. QH being a common and a more traditional device has better muscle adaptation and a lower risk of relapse. Despite this, it has few drawbacks. After the expander is soldered to molar bands, the cemented bands must be disengaged and re-cemented, or the expander must be adjusted intraorally. Despite this, the helices’ reputation as “flavor savers” stemmed from their ability to capture food particles.[15] This led to the introduction of the NHA, a cosy “non-food catcher” gadget made of round beta titanium wire that is 0.036” in diameter. It is simple to “fan expand” a V-shaped arch to straighten any upper first molar mesial rotation. The non-helix appliance can be modified to provide a distalizing force on the opposite molar, or even bilateral expansion and distalization, similar to the transpalatal arch that Cetlin introduced.[16] It is simple to separate the non-helix from the lingual sheath for activation or removal.[10]
Since, the non-helical palatal expander is a newly developed modification, there are not many studies carried out on the appliance till date. Hence, in this study, we have tried to evaluate the efficacy of the non-helical palatal expander versus the conventional quad helix in the correction of transverse discrepancy in growing patients. Hence, this study was carried out, in order to evaluate the clinical efficacy of the expansion appliance over a 6-month period, changes in occlusion – specifically, inter-canine, inter-premolar, and inter-molar widths; variations in arch lengths; and changes in incisor inclination – were studied. The pre- and post-treatment study models were thoroughly analyzed, leading to significant findings. In the sample group using the NHA, the mean inter-canine width increased from 29.1 mm pre-treatment to 31.8 mm post-treatment. In addition, statistical analysis showed an increase in the inter-premolar width with a mean difference of 2.320 ± 0.2426. The inter-molar width also improved, with mean pre- and post-treatment values of 38.1 mm and 42 mm, respectively. Al-Obaidi and Al-Mallah (2014)[17] stated that there was a significant difference in the rates of change for maxillary inter-1st premolar width, inter-2nd premolar width, and inter-1st molar width among the Hyrax expander, QH, and W-arch expander. However, no significant difference was observed between the QH and W-Arch expanders regarding these changes. Their analysis showed that the Hyrax appliance increased inter-premolar width by an average of 1.41 mm, while the QH and W-Arch appliances produced increases of 0.93 mm and 0.92 mm, respectively. The NHA also demonstrated an increase in arch length, resulting in alleviation of crowding, with a mean difference of 0.3333 ± 0.3086. Furthermore, there were no significant changes in proclination after NHA treatment, with pre- and post-treatment mean values of 6 and 5.9, respectively.
Shoaib et al.,[18] reported that following expansion, the maxillary arch perimeter significantly increased, averaging 6.9 mm for 9.1 mm of inter-molar width and an increase of 0.7 mm for each 1 mm of inter-molar expansion. According to Ladner and Muhl,[19] the posterior region of the maxilla experienced a more significant effect from expansion compared to the anterior region. Akkaya et al., (1999)[20] found similar values, indicating a ratio of approximately 0.7 mm for every 1 mm of expansion. In contrast, Berlocher et al., (1980)[21] recorded a 1 mm increase in arch size for every 1 mm of inter-molar expansion. Occlusal radiographic analysis confirmed similar changes in inter-arch width and arch perimeters. Vizzotto et al., (2007)[22] conducted a study measuring transversal widths through occlusal radiograph, with results aligning closely with those of Angelieri et al., (2013).[23] The paired samples t-test (P < 0.001) revealed that the mean increases in inter-canine and inter-molar widths were significantly greater for tipping (orthodontic effect) compared to suture opening (orthopedic effect). For the inter-canine region, the approximate ratio of sutural opening was 6:1, and for the intermolar area, it was 10:1.
The duration of the study was limited, preventing an assessment of the long-term stability and retention of the results. The study was conducted without gender discrimination, which means the effectiveness of the intervention may vary between genders. Another limitation was the relatively small sample size. A larger study group would have enhanced the authenticity of the findings. This study provides insights into the changes and efficacy of the NHA, with a primary focus on the active expansion that occurs during the treatment period. Future studies are needed to evaluate and investigate the retention and stability of the changes made post-expansion. In addition, further analysis of the expansion using 3D cone-beam computed tomography would aid in understanding the skeletal and dental changes achieved. This technology would also facilitate the visualization of mid-palatal suture opening. More research is necessary to compare the changes between different sexes.
CONCLUSION
The NHA group demonstrated significant palatal expansion in patients with transverse maxillary discrepancies. Measurements of inter-canine, inter-premolar, and inter-molar widths indicated a significant amount of expansion achieved by the NHA, as shown in both study models and occlusal radiographs. The arch perimeter exhibited positive changes due to the NHA, including de-crowding, changes in proclination and spacing. In summary, while this study effectively indicates the expansion brought about by the NHA, further research involving a larger sample size and a longer duration is required to assess the overall efficacy of this appliance in all three phases of orthodontic treatment.
Acknowledgments
We sincerely acknowledge and thank our subjects of the present study for participating and supporting constantly till the end of the study.
Author contributions
All the authors have contributed equally.
Ethical approval
The research/study approved by the Institutional Review Board at Rural Dental College, number 142, dated April 29, 2022.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Class II division 1 in new dimension: Role of posterior transverse interarch discrepancy in class II division 1 malocclusion during the mixed dentition period. J Clin Diagn Res. 2015;9:ZC72.
- [CrossRef] [PubMed] [Google Scholar]
- Dental arch width in Class II Division 2 deep-bite malocclusion. Am J Orthod Dentofacial Orthop. 2002;122:608-13.
- [CrossRef] [PubMed] [Google Scholar]
- Arch width changes in patients with Class II division 1 malocclusion treated with maxillary first premolar extraction and non-extraction method. J Clin Exp Dent. 2016;8:e403-8.
- [CrossRef] [PubMed] [Google Scholar]
- Role of posterior transverse interarch discrepancy in Class II, Division 1 malocclusion during the mixed dentition phase. Am J Orthod Dentofacial Orthop. 1996;110:417-22.
- [CrossRef] [PubMed] [Google Scholar]
- The role of rapid maxillary expansion in the promotion of oral and general health. Prog Orthod. 2015;16:33.
- [CrossRef] [PubMed] [Google Scholar]
- Early orthodontic treatment: What are the imperatives? J Am Dent Assoc. 2000;131:613-20.
- [CrossRef] [PubMed] [Google Scholar]
- Posterior cross-bites in the deciduous and mixed dentitions. Am J Orthod. 1969;56:491-504.
- [CrossRef] [PubMed] [Google Scholar]
- Longitudinal study and cost-benefit analysis of the effect of early treatment of posterior cross-bites in the primary dentition. Eur J Orthod. 1992;14:173-9.
- [CrossRef] [PubMed] [Google Scholar]
- The effects of maxillary expansion using a quad-helix appliance during the deciduous and mixed dentitions. Am J Orthod. 1981;79:152-61.
- [CrossRef] [PubMed] [Google Scholar]
- The postnatal development of the palatomaxillary region studied on human autopsy material. Am J Orthod. 1982;82:329-42.
- [CrossRef] [PubMed] [Google Scholar]
- Interview: Dr. Robert M. Ricketts on growth prediction 2. J Clin Orthod. 1975;9:340-9, 352
- [Google Scholar]
- A generalized treatment of irregularities. Paper read to section XII of the International Medical Congress. Trans Int Cong Med. 1881;3:542-7.
- [Google Scholar]
- The non-helix appliance: An alternative to the quad helix. J Clin Orthod. 2021;55:122-8.
- [Google Scholar]
- Comparison among three fixed palatal expander appliances: An in vitro study. Al-Rafidain Dent J. 2014;14:37-46.
- [CrossRef] [Google Scholar]
- Expansion changes by removable quad helix appliance on constricted maxilla in growing patients. Aust J Basic Appl Sci. 2017;11:171-7.
- [Google Scholar]
- Changes concurrent with orthodontic treatment when maxillary expansion is a primary goal. Am J Orthod Dentofacial Orthop. 1995;108:184-93.
- [CrossRef] [PubMed] [Google Scholar]
- A comparison of sagittal and vertical effects between bonded rapid and slow maxillary expansion procedures. Eur J Orthod. 1999;21:175-80.
- [CrossRef] [PubMed] [Google Scholar]
- The effect of maxillary palatal expansion on the primary dental arch circumference. Pediatr Dent. 1980;2:27-30.
- [Google Scholar]
- The Quad-Helix appliance in the primary dentitionorthodontic and orthopedic measurements. J Clin Pediatr Dent. 2007;32:165-70.
- [CrossRef] [PubMed] [Google Scholar]
- Midpalatal suture maturation: classification method for individual assessment before rapid maxillary expansion. Am J Orthod Dentofacial Orthop. 2013;144:759-69.
- [CrossRef] [PubMed] [Google Scholar]




