
Innovative and simple technique of stabilizing the lingual retainer wire before bonding

*Corresponding author: Pradnya Atish Korwar, Department of Orthodontics and Dentofacial Orthopedics, Mahatma Gandhi Mission’s Dental College and Hospital, Navi Mumbai, Maharashtra, India. dr.pradnya1987@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Korwar PA, Gheware A, Ravindranath VK. Innovative and simple technique of stabilizing the lingual retainer wire before bonding. J Global Oral Health. 2024;7:54-6. doi: 10.25259/JGOH_40_2023
Abstract
Long-term stability of orthodontic treatment outcome is attained through retention. Fabrication and bonding of the lingually bonded retainer on the lingual tooth surface are a technique-sensitive and time-consuming procedure. Stabilizing the lingual retainer wire on the tooth surface throughout the bonding procedure is a challenging task for the operator. This article introduces a new simplified technique of stabilizing the lingual retainer wire before bonding.
Keywords
Lingual bonded retainer
Fixed retainer
Bonding
Retention
Dental floss

INTRODUCTION
Orthodontists aim to achieve long-term stability of orthodontic treatment outcomes through retention. One of the most commonly used retention appliances is the lingual bonded retainer (LBR) because it is imperceptible, inconspicuous, well tolerated, and effective in maintaining treatment outcomes with minimal patient compliance.[1-3] Nevertheless, fabrication and bonding of the LBR passively on the lingual tooth surface are a technique-sensitive and time-consuming procedure[4-6] that requires correct isolation and bonding procedures. Furthermore, stabilizing the lingual retainer on the tooth surface during bonding is a challenging task for the operator. The rationale of this article is to introduce a new simplified technique of stabilizing the lingual retainer wire preceding the bonding procedure in finished orthodontic cases. The aim of this technique is to simplify the clinical process and to reduce the chair side time involved in bonding the LBR.
TECHNIQUE
A stem of elastomeric ligature ties, dental floss, a needle with eye hole, metal scissors, bracket-holding tweezers, and needle-holding forceps [Figure 1]. Take a stem of elastomeric ligature ties and cut it into pieces of about 4-mm thickness with metal scissors. A stem of elastomeric ligature ties is used as this part has enough flexibility to allow piercing with a needle and firmness for a strong grip on dental floss when tightened. Double thread a piece of dental floss about 4 inches through the eye hole of a needle and pierce the needle through the sectioned piece of stem of elastomeric ligature ties with the help of needle-holding forceps and bracket-holding tweezers. Remove the needle and tie the loose ends of the floss [Figure 2]. Prepare the teeth for fixed retainer bonding by oral prophylaxis, cheek retractor, saliva ejector, and cotton rolls in place. Etch and prime the palatal/lingual surface of the teeth. Take the above-fabricated floss and pass one end of the floss loop interdentally between the lateral incisor and canine (or between the terminal teeth as per preference) on both sides and between the central incisors as well if required. Cut the multi-braided retainer wire as per requirement and pass through the floss loops lingually. Tighten the floss loops by pulling the elastomeric piece toward the interdental area of the teeth so that the retainer wire is held firmly over the lingual surface. Adapt it as desired by checking interocclusal interferences. Apply and cure flowable composite. Loosen, cut the floss loops with scissors, and remove them [Figure 3].

- The armamentarium required: (a) Stem of elastomeric ligature ties. (b) Dental floss. (c) Needle with eyehole. (d) Metal scissors. (e) Bracket holding tweezers. (f) Needle-holding forceps.
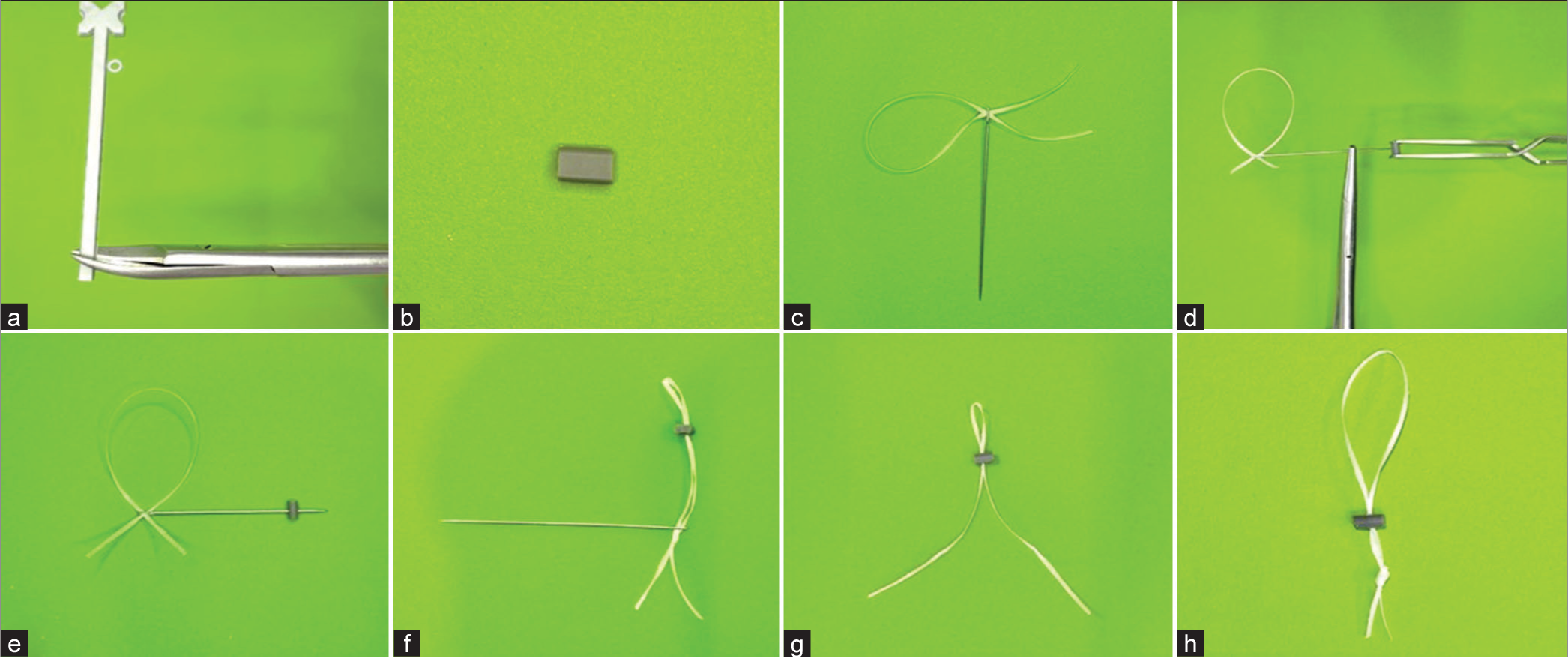
- (a) Take a stem of elastomeric ligature ties and cut it into pieces of about 4-mm thickness with metal scissors. (b) Sectioned piece of the stem of elastomeric ligature ties. (c) Double thread a piece of dental floss about 4 inches through the eyehole of a needle. (d) Firmly take a grip on the needle with needle-holding forceps and sectioned elastomeric piece with a bracket holding tweezers. (e) Pierce the needle through the elastomeric piece. (f) Straighten the floss. (g) Remove the needle from the floss. (h) Tie the loose ends of the floss.
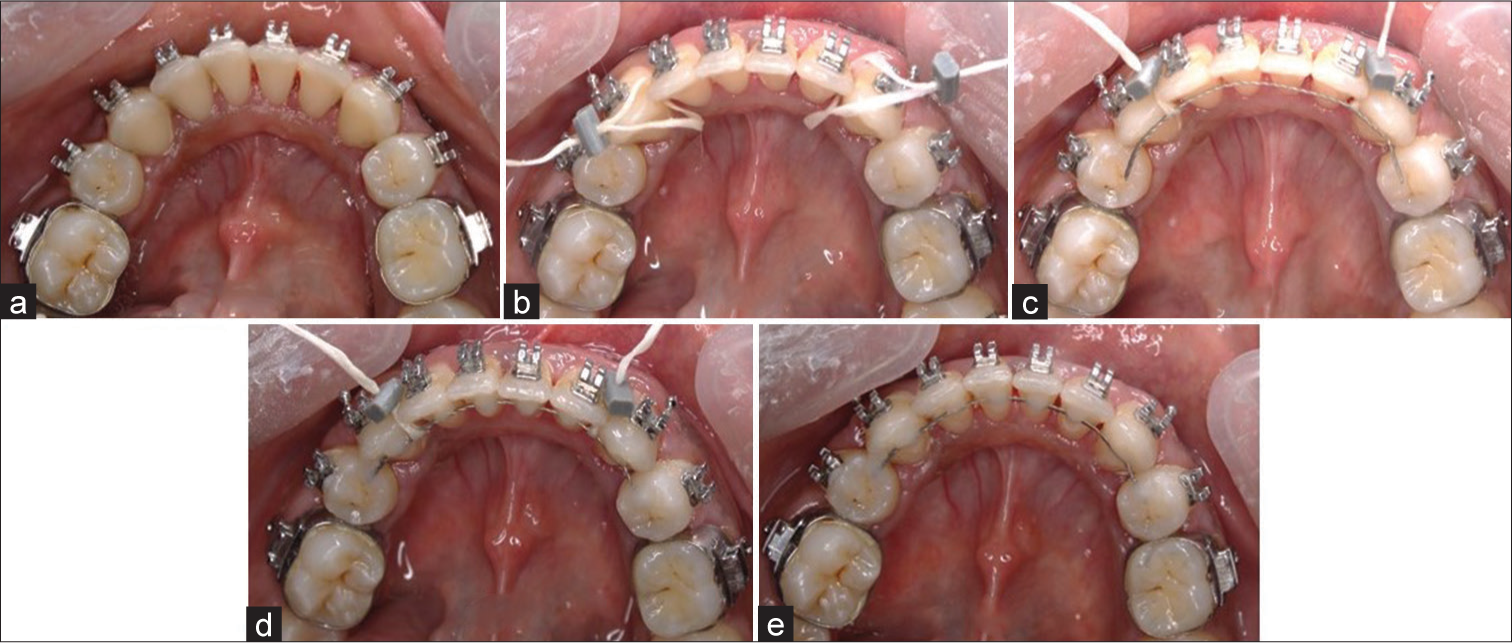
- (a) Mandibular teeth prepared for fixed retainer bonding. (b) One end of the floss loop is passed interdentally between the lateral incisor and canine on both sides. (c) Multi-braided retainer wire is sectioned and passed through the floss loops lingually, the floss loops are tightened by pulling the elastomeric piece toward the interdental area of the teeth, and the wire is adapted by checking interocclusal interferences. (d) Flowable composite is applied and cured. (e) Floss loops are loosened, cut with scissors, and removed.
DISCUSSION
Retention is a critical phase of orthodontic treatment to prevent relapse. There are various retention appliances available including removable retainers and fixed bonded retainers. Removable retainers have their own advantages and disadvantages, but they require the patient’s compliance to use them. Fixed retainers consist of a piece of orthodontic wire that is bonded on the lingual surface of the tooth.[5] The main advantages of fixed retainers are invisibility, minimal patient compliance, and long-term retention. Although fixed retainers are advantageous, bonding a lingual retainer is a challenging and technically sensitive procedure, as their placement requires a longer working time, there is a risk of contamination by saliva, the adaptation of the retainer wire to the lingual surface of the anterior teeth is difficult,[2] and their stabilization during bonding is, therefore, a tedious task. If retainer wire is effectively stabilized over the palatal/lingual surface of teeth, bonding becomes a simple process. Hence, various materials to stabilize the lingual retainer before bonding are used.[7] Many direct methods have been developed using fingers, dental floss, orthodontic wires, elastics, ligatures, and others to stabilize the retainer wire, but these methods have certain shortcomings.[1,4]
Dental floss is widely used to stabilize LBR before bonding. However, it requires the use of artery forceps to hold the floss interdentally which in turn requires assistance from another person. The technique described here is a simple method for stabilizing the lingual retainer wire on the palatal/lingual surface of the teeth without causing iatrogenic damage to the adjacent soft tissues when bonding the LBR it is a reliable, simple, time-saving, and economical procedure as it does not require any special equipment, be executed with the use of materials that are easily available in any dental setup and can be done single-handedly by the clinician.
CONCLUSION
This is a simple and effective way of stabilizing the lingual fixed retainer before bonding, which will reduce chairside time in its placement, thereby reducing the chances of contamination and bond failure leading to effective retention of post-treatment results.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Clinical experience with direct-bonded orthodontic retainers. Am J Orthod. 1977;71:440-8.
- [CrossRef] [PubMed] [Google Scholar]
- Effectiveness of lingual retainers bonded to the canines in preventing mandibular incisor relapse. Am J Orthod Dentofacial Orthop. 2008;134:179.e1-8.
- [CrossRef] [Google Scholar]
- Inadvertent tooth movement with fixed lingual retainers. Am J Orthod Dentofacial Orthop. 2016;149:277-86.
- [CrossRef] [PubMed] [Google Scholar]
- The bonded lingual retainer and multiple spacing of anterior teeth. Swed Dent J Suppl. 1982;15:247-55.
- [Google Scholar]
- Bonded orthodontic retainers: A review. Am J Orthod Dentofacial Orthop. 1995;108:207-13.
- [CrossRef] [PubMed] [Google Scholar]
- Two-year survival analysis of twisted wire fixed retainer versus spiral wire and fiber-reinforced composite retainers: A preliminary explorative single-blind randomized clinical trial. Korean J Orthod. 2016;46:104-10.
- [CrossRef] [PubMed] [Google Scholar]




