
An emerging new variant of tobacco – A pilot study

*Corresponding author: R. Dharshanram, Department of Public Health Dentistry, Ragas Dental College, Chennai, Tamil Nadu, India. ram.dharu14@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Dharshanram R, Madankumar PD. An emerging new variant of tobacco – A pilot study. J Global Oral Health 2020;3(1):14-7.
Abstract
Objectives:
The tobacco epidemic is one of the biggest public health threats, the world has ever faced and more than 6 million of those deaths are the result of direct tobacco use. Chewing tobacco is a type of finely cut and ground, dried form of smokeless tobacco product. It is commonly and idiomatically known by various terms most often as chew. In addition, it is also widespread in the migrant populations from Indian states such as Andhra Pradesh, Bihar, Gujarat, Karnataka, Maharashtra, Odisha, and Telangana. Aim of this study was to assess the prevalence of the new variant of tobacco (BONDAKUTCHI), among population being surveyed at Ranipet, Tamil Nadu.
Materials and Methods:
A cross-sectional study was conducted at Thirumalai Mission Hospital, Ranipet, Vellore. We mainly focused on a group of participants who are from zone 1. Convenience sample of 62 participants within the age group of 20–80-year-old population and both males and females were included in the study. Oral health status was assessed using the WHO pro forma (2013) and Fagerstrom test for nicotine dependence. Scales for smokeless tobacco used to assess the nicotine dependency.
Results:
Among 62 participants, 38 were male and 24 were female. The mean age of this participant was 45.20 ± 11.03 years. Among the 62 participants, 62% of the population had a habit of using the new variant of tobacco products.
Conclusion:
While legislators should consider enforcing and extending existing tobacco laws to a growing new variant of tobacco, further research is required to fill gaps in the literature and provide evidence based interventions for tobacco control specialists and health-care professionals.
Keywords
Bondakutchi
Smokeless tobacco
New variant of tobacco
Vellore
Prevalence

INTRODUCTION
The tobacco epidemic is one of the biggest public health threats, the world has ever faced and more than 6 million of those deaths are the result of direct tobacco use (World Health Organization).[1] According to the Global Adult Tobacco Survey (GATS) 2016–2017, 29.6% of men, 12.8% of women, and 21.4% (199.4 million) of all adults currently use smokeless tobacco (SLT).[2] With recent government policies restricting the sale and use of tobacco products coupled with the recent ban on production of smokeless tobacco products in many Indian states, there is an emerging trend of newer surrogate tobacco products as alternative to the traditionally used ones.
There is a wide variation in smokeless tobacco use prevalence at subnational level in most of the countries in the region. In India, such variation is very wide.[3] The India GATS (2016–17) showed that nationally, over a quarter of Indians aged 15 and above use smokeless tobacco products (26%), but the prevalence ranges from about 5% in Himachal Pradesh and Goa to nearly 50% in Bihar, Jharkhand, and Chhattisgarh. The proportion of men using smokeless tobacco was the highest in Bihar (62.2%) and lowest in Goa and Pondicherry (6%). Women in the northeastern states of Mizoram (49%) and Tripura (43.5%) used smokeless tobacco products the most, while there was almost a negligible use of SLT among women in Punjab (0.6%) and Himachal Pradesh (0.2%).[4]
Chewing tobacco is a type of finely cut and ground, dried form of smokeless tobacco product. It is commonly and idiomatically known by various terms most often as chew.[5] In addition, it is also widespread in the migrant populations from Indian states such as Andhra Pradesh, Bihar, Gujarat, Karnataka, Maharashtra, Odisha, and Telangana. This type of new variant of tobacco (BONDAKUTCHI) [Figures 1 and 2] does not come under the Cigarettes and Other Tobacco Products Act.[6]

- New variant of tobacco (BONDAKUTCHI).

- Clinical picture of new variant of tobacco (BONDAKUTCHI) users.
With these consequences, we hereby conduct a pilot study, the aim of this study was to assess the prevalence of the new variant of tobacco (BONDAKUTCHI), among population being surveyed at Ranipet, Tamil Nadu, India.
MATERIALS AND METHODS
This cross-sectional study was conducted at Thirumalai Mission Hospital, Ranipet, Vellore. We mainly focused on a group of participants who are from zone 1 (which covered seven villages, Thalangai, Ranipet, Jolarpet, Thozhupedu, Ammoor, Velam, and Kalpudur). Survey was done in area which the Oral Health Screening Program covered. This study was conducted in the period of 3 months (January–March 2019). Convenience sample of 62 participants within the age group of 20-80 year population and both males and females were included in the study. Participants with severe levels of disorientation, other products of smokeless tobacco users, smoking tobacco users, and alcohol users under any cessation treatment or positive breath alcohol level at any session were excluded from the study. Self-reported demographic data questionnaire was administrated among the study participants. Oral health status was assessed using the WHO pro forma (2013) and Fagerstrom test for nicotine dependence (FTND). Scales for smokeless tobacco used to assess the nicotine dependency. Procedures were approved by the Institutional Review Board (ethical clearance number RDC-54/2018) and written informed consent was obtained from all participants.
Statistical analysis
Data entry was done using Microsoft Excel 2007; statistical analysis was done using IBM SPSS version 19 for descriptive statistics.
RESULTS
Among 62 participants, 38 were male and 24 were female. The mean age of this participant was 45.20 ± 11.03 years. Among the 62 participants, 62% of the population had a habit of using the new variant of tobacco products [Figure 3]. The mean FTND score was 3.80 ± 1.63 and females had a higher nicotine dependency than males. Females had 3.03 ± 1.50 and males had 2.95 ± 1.20 [Table 1].
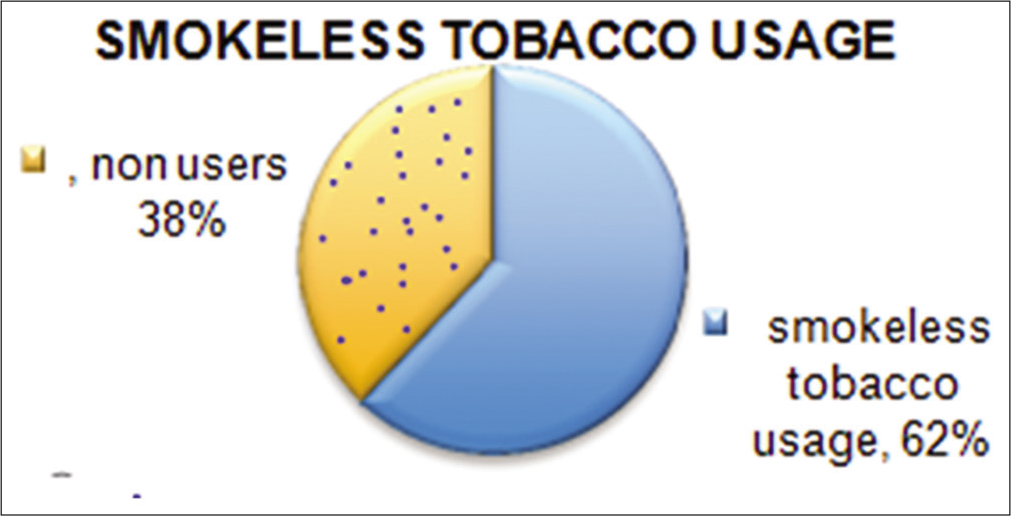
- Frequency distribution of new variant of tobacco users.
| Demographic characteristics | ||
|---|---|---|
| Total number of participants | n=62 (Male – 38, female – 24) | |
| Education | High school (n=54), intermediate, post high school (n=6), graduate/Postgraduate (n=2), profession/honors (n=0) | |
| Occupation | Unemployed (n=32), semiskilled (n=12), skilled (n=9), unskilled (n=9) | |
| Monthly income (in INR) | 2181–6477 (n=46), 6478–10,795 (n=15), 10,796–16,193 (n=1), 16,194–21,591 (n=0),21,592–43,183 (n=0) | |
| Socioeconomic status (Kuppuswamy scale –2016) | Upper lower (n=5), middle (n=8), lower (n=49) | |
| Mean | SD | |
| Age (years) | 48.10 | 9.03 |
| Fagerstrom test for nicotine dependence score | 3.80 | 1.63 |
| Male | 2.95 | 1.20 |
| Female | 3.03 | 1.50 |
In this study, mean distribution scores of decayed, missing, and filled teeth (DMFT) showed that study populations with the habit of smokeless tobacco usage had a lower DMFT score of 5.10. In this study periodontal status assessment among new variant of tobacco products (BONDAKUTCHI) users which was revealed that the lower mean number of teeth with gingival bleeding and periodontal pocket (0.31 ± 0.16) and (0.22 + 0.16) respectively. The mean score loss of attachment was higher among the study population (1.28 + 0.45). Most of the study participants have no sign of dental erosion (67.7%) and dental trauma (12.9%) [Tables 2 and 3]. The mean score loss of attachment was higher among the study population (1.28 + 0.45) [Table 4].
| Score | Dental erosion | Dental trauma | ||
|---|---|---|---|---|
| Frequency | Percentage | Frequency | Percentage | |
| 0 | 12 | 19.3 | 46 | 74.1 |
| 1 | 8 | 12.9 | 8 | 12.9 |
| 2 | 42 | 67.7 | 8 | 12.9 |
Dental erosion score 0: No sign of erosion, 1: Enamel lesion, 2: Dentinal lesion;
Dental trauma score 0: No sign of injury, 1: Treated injury, 2: Enamel fracture only
| Variable | n | Mean±SD | Minimum | Maximum |
|---|---|---|---|---|
| Gingival bleeding | 62 | 0.31±0.16 | 0.12 | 0.70 |
| Pockets | 62 | 0.22±0.16 | 0.00 | 0.60 |
| Loss of attachment | 62 | 1.27±0.35 | 1.00 | 2.00 |
| DMFT – smokeless tobacco users | 62 | 5.10±0.23 | 3.00 | 8.00 |
| DMFT – non-users | 6.40±0.78 | 5.00 | 9.00 |
DMFT: Decayed, missing, and filled teeth
| LOA | Frequency | Percentage |
|---|---|---|
| 4–5 mm | 55 | 88.7 |
| 6–8 mm | 7 | 11.2 |
LOA: Loss of attachment
Frequency distributions of intervention urgency among participants are given in [Table 5]. Among the study participants of patients, 67.7% need preventive treatment and 14.5% need prompt treatment including scaling and 12.9% need preventive routine treatment.
| IU | Frequency | Percentage |
|---|---|---|
| 0 | 3 | 4.8 |
| 1 | 42 | 67.7 |
| 2 | 9 | 14.5 |
| 3 | 8 | 12.9 |
IU: Intervention urgency
DISCUSSION
Smokeless tobacco use may be of two kinds: Oral use and nasal use. In India and Southeast Asia, nasal use is uncommon.[7] In South India, usage of emerging new variants of tobacco as alternatives for banned smokeless tobacco and smoking tobacco is growing on a day to day basis.[8]
Trend data on the prevalence of smokeless tobacco use are not available, but inferences may be drawn from the data on total tobacco consumption.[9] Therefore, only oral use of new variant of tobacco (BONDAKUTCHI) is described in this paper. Our study is an initial attempt to assess the prevalence of new variant of tobacco.
New variant of tobacco is a dried stem of Nicotiana tabacum. Stem is under a process of flue-curing which is a heat-driven process that creates a dry manageable product, reduces the risk of mold, and promotes chemical changes that improve the sensory quality. It also produces a change in stem color which is blackish to brown color. Dried stem of tobacco plant (principle investigator personal preference) has more of the spice/burn sensation and natural flavor of this product was brown roasted maple woody bitter. Patients have a sense of high level of satisfaction and dependence characteristically attributing this to better taste which is less spicy than other smokeless tobacco and cost factor of this product.
It is prepared in rural areas and is not available in the commercial markets. In India, the tax rate of 28% and ad valorem cess of 5% remain the same except in the case of other items falling in the cigarette category and tobacco products.[10] These types of sales and works come under small-scale industry which is not applicable for goods and service taxes. Hence, it is extremely cheap and easily available at local shops.
Screening program comprises three zones, each zone has 18 villages. From the 18 villages, we selected one village and conducted a pilot study for assessing the prevalence of usage of new variant of tobacco. Sixty-two study participants were a part of this study.
Among the 62 participants, 62% of the population had a habit of using the new variant of tobacco products. Female participants have a higher nicotine dependency than males. The available evidence suggests a higher prevalence and severity of periodontal diseases among patients as compared to the general population. According to the GATS survey, there was negligible use of smokeless tobacco (BONDAKUTCHI) among women as opposed to our study, which showed that females have higher nicotine dependency than males.
CONCLUSION
New variant of smokeless tobacco use (BONDAKUTCHI) appears to be on the increase, especially among older users, and therefore represents a potential public health concern. While legislators should consider enforcing and extending existing tobacco laws to a growing new variant of tobacco, further research is required to fill gaps in the literature and provides evidence-based interventions for tobacco control specialists and health-care professionals. Strong and sustainable measures need to be incorporated both by civic administration and public health departments for its forceful implementation.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- World Health Organization Reports. 2019. Available from: https://www.who.int/news-room/fact-sheets/detail/tobacco [Last accessed on 2019 Aug 23]
- [Google Scholar]
- International Institute for Population Sciences. Ministry of Health and Family Welfare, Government of India (2009-2010) In: Global Adult Tobacco Survey India (GATS India). India: International Institute for Population Sciences; 2010.
- [Google Scholar]
- Prevalence and determinants of tobacco use in India: Evidence from recent global adult tobacco survey data. PLoS One. 2014;9:e114073.
- [CrossRef] [PubMed] [Google Scholar]
- International Institute for Population Sciences. Ministry of Health and Family Welfare, Government of India (2009-2010) In: Global Adult Tobacco Survey India (GATS India). India: International Institute for Population Sciences; 2017.
- [Google Scholar]
- WHO Report on Trends in Prevalence of Tobacco Smoking 2000-2025 (2nd ed). Geneva: World Health Organization; 2018.
- [Google Scholar]
- Sociocultural diversity and substance use pattern in Arunachal Pradesh, India. Drug Alcohol Depend. 2004;74:97-104.
- [CrossRef] [PubMed] [Google Scholar]
- Smokeless tobacco use is “replacing” the smoking epidemic in the South-East Asia region. Nicotine Tob Res. 2019;21:95-100.
- [CrossRef] [PubMed] [Google Scholar]
- World Health Organization Report. 2006. Available from: https://www.who.int/tobacco/communications/events/wntd/2006/report_v8_4may06.pdf [Last accessed on 2019 Aug 24]
- [Google Scholar]
- Commonly Used Smokeless Tobacco Products Around the Globe. 2019. World health Organization Convention, ICMR. Available from: https://www.untobaccocontrol.org/kh/smokeless-tobacco/paan-betel-quid-tobacco [Last accessed on 2019 Aug 24]
- [Google Scholar]
- Available from: https://www.economictimes.indiatimes.com/news/economy/policy/gst-council-decides-to-hike-cess-on-cigarettes/articleshow/59635800.cms?from=mdr [Last accessed on 2019 Aug 23]




