
Translate this page into:
Effectiveness of coconut oil pulling as an adjuvant to oral hygiene procedure on plaque-induced gingivitis among middle-aged adults – An interventional study

-
Received: ,
Accepted: ,
How to cite this article: Menaka V, Kavya G, Bhuvaneshwari R, Azali AS, Aparna S, Kumar PD. Effectiveness of coconut oil pulling as an adjuvant to oral hygiene procedure on plaque-induced gingivitis among middle-aged adults – An interventional study. J Global Oral Health 2019;2(2):102-7.
Abstract
Objectives:
Oral health correlates with systemic health, and maintaining oral health is very important because the oral cavity is considered as a reflection of the general well-being of a human body. Daily plaque removal with a toothbrush is an important component of most oral hygiene programs intended to prevent and control two globally leading oral afflictions dental caries and periodontal diseases. Failure to comply and lack of technical skills of the patient has lessened the effectiveness of conventional tooth brushing. Because of this, research efforts have focused on adjuvant therapy along with brushing for reducing and controlling plaque-induced oral diseases. One such measure is oil pulling. Oil pulling has been used extensively as a traditional Indian folk remedy for many years to prevent decay, oral malodor, bleeding gums, dryness of throat, cracked lips, etc. Most of the studies have been done using sesame oil. Since coconut oil also has many health effects such as boosting the immune system and antimicrobial properties, this can also help in fighting against various pathogens of oral cavity that will in turn act as an effective plaque control agent. Hence, with this background, this study is contemplated to evaluate the benefit of oil pulling along with normal brushing techniques in adults under the age group of 35–44 years.
Materials and Methods:
Forty healthy subjects belonging to both the sexes who presented with plaque-induced gingivitis will be selected for the study and will be divided into control and study groups. The patients will be informed about the nature and purpose of the study. Health education will be provided to all the students. The modified bass technique will be demonstrated to the participants and they are directed to brush twice daily for 3 min. Toothbrush and toothpaste will be provided to all participants. Among them, 20 subjects were instructed to continue their normal oral hygiene procedures along with coconut oil pulling. Data collected were subjected to appropriate statistical tests using SPSS version 20.
Results:
A highly statistical difference was seen between the two groups and within the groups.
Conclusion:
The usage of coconut oil pulling as an adjuvant to oral hygiene gives a promising result.
Keywords
Plaque
Periodontal diseases
Gingivitis
Oil
Coconut

INTRODUCTION
Oral health is a fundamental and integral part of general health and is considered a prime importance to all individuals. Dental caries and periodontal diseases are the two globally leading oral afflictions which can be effectively prevented and controlled by an effective plaque control method.[1] Apart from the usage of mechanical tooth cleaning to maintain oral health, research has focused on chemotherapeutic agents such as mouthwash containing chlorhexidine as an adjuvant to reduce plaque formation in the oral cavity. However, these chemotherapeutic agents have certain undesirable adverse effects which have led to several other alternatives, among which oil pulling procedure is one of the alternatives which can readily be made available in the household. Oil pulling is the natural folk remedy from India that has been practiced as a holistic Ayurvedic technique which has been mentioned in the textbooks written by Charaka and Susrutha and it has been beneficial for about 30 different illnesses including diabetes, asthma, headache, and migraine.
According to the study conducted by the World Health Organization, 80% of people in India have been using herbal medicine to improve their health.[2] Oil pulling therapy can be done using sunflower or sesame oil with coconut oil being commonly used in various studies.[3] Since coconut oil also has health benefits such as boosting the immune system and antimicrobial properties, it can also be used in the fight against various pathogens of the oral cavity which can in turn act as an effective plaque control agent. It is the act of the oil pulling which nullifies the toxins and other microbes from various parts of the oral cavity. Coconut oil is one such type of oil that is highly absorbable with multiple health benefits such as reducing inflammation, improving gum health, fighting bacteria, reducing bad breath, and preventing dental caries. In oil pulling using coconut oil, the chances of toxicity in case of ingestion are low since it is edible.
Evidence showed that coconut oil has significant antimicrobial activity against Escherichia vulneris, Enterobacter spp., Helicobacter pylori, Staphylococcus aureus, and Candida spp., including Candida albicans, Candida glabrata, Candida tropicalis, Candida parapsilosis, Candida stellatoidea, and Candida krusei.[4] It was hypothesized that monolaurin and other medium-chain fatty acids have the capacity to alter bacterial cell wall, penetrate and disrupt cell membranes, inhibit enzymes involved in energy production and nutrient transfer, causing death of the bacteria thus explaining the antibacterial action of coconut oil. Literature has shown that simply holding or swishing comfortable amount of oil in the mouth for 10–15 min and spitting it out has an antibacterial effect. Although studies have reported systemic health benefits of coconut oil, there is a dearth of evidence reporting the oral health benefits of coconut oil pulling. Hence, the present study was conducted to assess the effect of coconut oil on plaque formation and plaque-related gingivitis among middle-aged adults in Chennai.
MATERIALS AND METHODS
An interventional, single-blinded study was conducted in Kovalam, Chennai that included a group of adults ranging from the age of 35 to 44 years old. The ethical clearance for the study was obtained by the Institutional Review Board, Ragas Dental College and Hospital, and the study was registered under the Clinical Trial Registry of India with the register number (CTRI/2019/12/022393). The subjects were informed about the nature, purpose of the study and their adverse effects and complications from the samples being investigated and written informed consent was obtained from all subjects. The inclusion criteria included subjects who had severe gingivitis based on Loe and Silness Gingival Index (1963) and poor PLI score based on modified Silness and Loe plaque index (1967). The subject under orthodontic treatment and those with systemic diseases and are using antibiotics were not included in the study and subjects who are currently using mouth wash as an adjuvant to oral hygiene were excluded from the study. A total of 40 individuals with an age range of 35–45 years old fulfilling the above-mentioned criteria were selected and randomly allocated to the groups. Each subject was assigned a specific number and simple random sampling was done using a table of random numbers. Group A (cases) included 20 subjects who were instructed to do normal tooth brushing along with coconut oil pulling. Group B (control) included 20 subjects who were instructed to do only normal tooth brushing.
Gingival Index by Loe and Silness (1963) was used to assess the severity of gingivitis on the index teeth 16, 12, 24, 36, 32, and 44. The tissues surrounding each tooth were divided into four gingival scoring units, distofacial papilla, facial margin, mesiofacial papilla, and the entire lingual gingival margin. A blunt instrument, such as a periodontal pocket probe, was used to assess the bleeding potential of the tissues.
Modified plaque index by Loe and Silness (1967) was used to assess the thickness of plaque on the gingival one-third of the index teeth 16, 12, 24, 36, 32, and 44. The area to be examined is divided into four areas which are distofacial, facial, mesiofacial, and lingual surface of the tooth. Totaling the scores around each tooth gave the gingival index score and plaque index score for the area. Totaling all the scores and dividing by the number of teeth examined provided the gingival index score and plaque index score for that person and was interpreted accordingly.
For oil pulling therapy, the subjects were advised to take 10 ml of coconut oil (Tendders Wonders Gandoosha Thaila® [Tendders Wonders LLP] that are made of purely tender coconut and the highest concentration of lauric acid without the addition of any preservatives). They were asked to sip, suck, and pull the oil through the teeth and they had to lift their chin a bit, close their eyes and start swishing liquid from left to right, front to back, and vice versa. After 2 min, when the oil became milky white, thin, and frothy, they were asked to spit the liquid. The oil pulling procedure was followed by brushing the teeth and was advised preferably on an empty stomach in the morning. A demonstration of a modified bass technique was given to the participants of both the groups. Group A was directed to brush twice daily for 3 min and was advised to routinely perform oil pulling with coconut oil every day in the morning. Participants in Group B were advised to perform routine tooth brushing. Toothbrush and toothpaste were provided to all participants. None of the subjects discontinued from the study showing good compliance.
A baseline assessment was done using the gingival index (Loe and Silness, 1963) and modified plaque index (Silness and Loe, 1967). After 6 weeks, gingival bleeding and plaque deposition were assessed using the same indices and compared.
Calibration of the examiner
The examiner was adequately trained for scoring indices and providing oral health education aids at the Department of Public Health Dentistry, Ragas Dental College and Hospital, Chennai, under the supervision of the Head of the Department. The calibrated examiner recorded all the indices such as the gingival index and modified plaque index.

Statistical analysis
Data were grouped into a Microsoft Excel table and further analyzed using the Statistical Package for the Social Sciences (SPSS) 20.0 and Microsoft Word and Excel have been used to generate graphs.
RESULTS
The graph [Figures 1 and 2] shows a comparison between the baseline values of the mean gingival index and mean plaque index between Group A and Group B. There was no significant difference between the scores at baseline indicating that the baseline mean values of both the groups were the same. The comparison was again done after 6 weeks of study between the mean gingival index and plaque index in Groups A and B, where the graphs show a significant difference between the two groups. As shown in Tables 1 and 2, there was a significant reduction in both mean gingival index and plaque index of Group A with mean ranging from 1.496 to 0.68 (mean gingival index) and 1.885 to 1.102 (mean plaque index) whereas in Group B, the mean value showed no statically significant reduction.
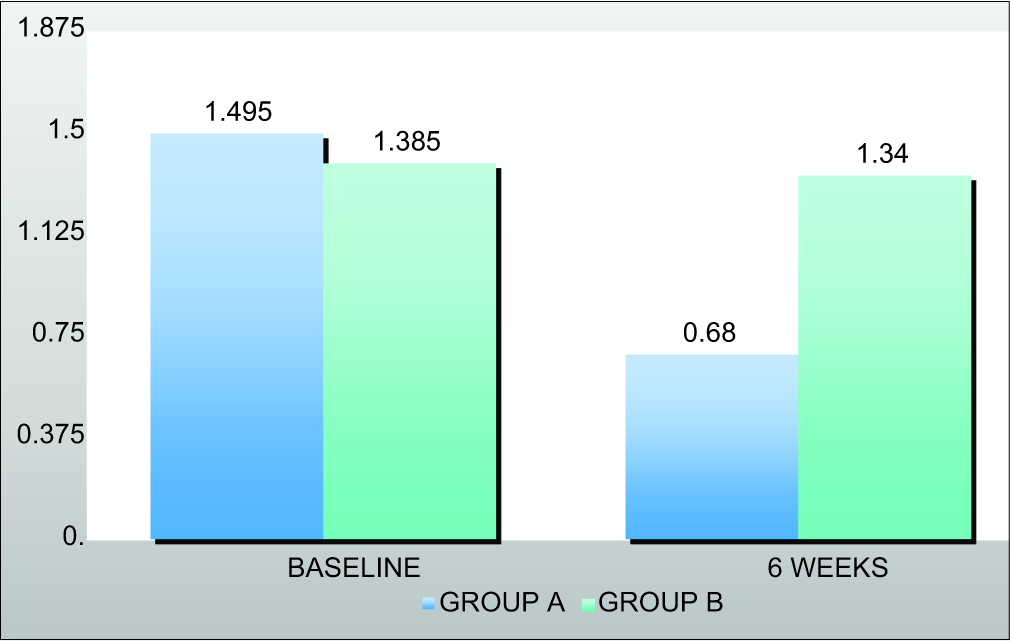
- Mean gingival index.
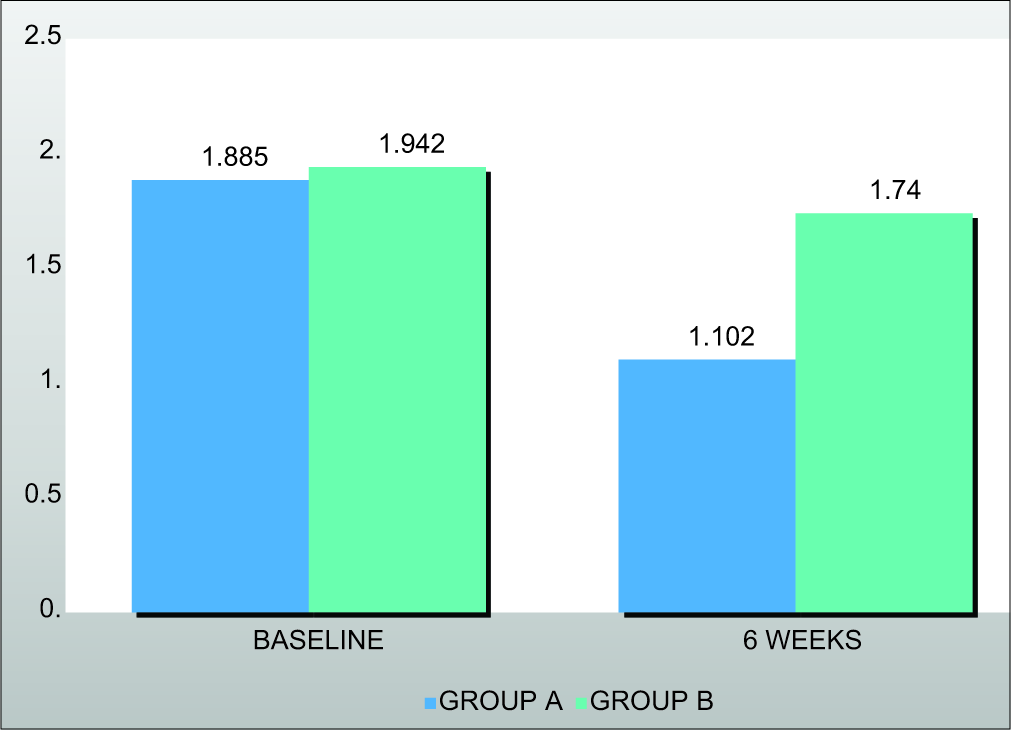
- Mean plaque index.
| Group A | Group B | P-value | |
|---|---|---|---|
| Baseline | 1.495 | 1.385 | 0.433 |
| 6 weeks | 0.68 | 1.34 | 0.000 |
| P-value | 0.000 | 0.789 |
| Group A | Group B | P-value | |
|---|---|---|---|
| Baseline | 1.885 | 1.942 | 0.256 |
| 6 weeks | 1.102 | 1.74 | 0.000 |
| P-value | 0.000 | 0.03 |
DISCUSSION
Plaque-induced gingivitis is the most common form of the gingival disease and is the result of an interaction between microorganisms found in the dental plaque biofilm and the tissues and inflammatory cells of the host. Ayurveda, a part of alternative medicine, is gaining back its importance in various aspects of health, as it uses all natural products. Oil pulling is one such age-old process which has innumerable systemic and dental health benefits as it holds that each section of the tongue is connected to different organs such as to the kidneys, lungs, liver, heart, small intestines, stomach, colon, and spine. It has become a mystic cure for many systemic diseases such as diabetes and migraine.[5] Oil pulling is a folk remedy which has certain benefits over commercially available mouth rinses as reported in a systematic review by Bekeleski et al. in 2012.[6] The exciting aspect of this healing method is its simplicity.
A systematic review by Gbinigie et al. in 2016[7] found that oil pulling might be as effective as chlorhexidine mouthwash in reducing plaque. Chlorhexidine-containing mouthwashes have been widely considered as the “gold standard” among other topically applied agents, but it may discourage compliance because of its unpleasant taste and undesirable side effects, such as tooth staining and alterations in taste sensations. The results of this study hold promise in reducing plaque and gingivitis without negative side effects such as staining, altered taste but cost-effective and better patient compliance.
Coconut oil contains predominantly medium-chain fatty acids, as shown in Table 3 of which 45–50% include lauric acid which is known for its anti-inflammatory and antimicrobial properties. The long-chain fatty acids present in other oils are not easily metabolized as medium-chain fatty acids, and hence stored as fat. Various hypotheses have been put forward regarding the mechanism of action of oil pulling like the oil swishing action which generates mechanical shear forces due to agitation and results in the emulsification of oil thereby increasing the surface area of oil which can reduce plaque adhesion and bacterial coaggregation. Furthermore, alkali in saliva reacts with oil to result in saponification or soap-like substance formation which has a cleansing action. The potential downside for patients using oil pulling is lipoid pneumonia due to its aspiration and the extended duration of the procedure.[8]
| Fatty acids | Percentage |
|---|---|
| Lauric | 45–50 |
| Myristic | 13–19 |
| Palmitic | 8–11 |
| Capric | 6–10 |
| Caprylic | 5–9 |
| Oleic | 5–8 |
| Stearic | 1–3 |
| Linoleic | <3 |
| Caproic | <1 |
Oil pulling can be a supplemental oral hygiene aid but cannot be considered as a replacement for tooth brushing. However, toothbrushing may be contraindicated in certain cases of mouth ulcers, fever or indigestion or in those who have a tendency to vomit, have asthma or cough. Oil pulling therapy can be used to clean the oral cavity in all these cases. Reduction in percentage sites with visible plaque was found to be 8% in the manual toothbrush group and 30% in the electric toothbrush group and the mean reduction in gingivitis was 8% and 9% after 6 weeks.[9] The results are in concurrence with our study, except for the fact that oil pulling has resulted in a far greater reduction in gingivitis, than the manual toothbrushes.[1]
The results of our study are in line with Chalke et al. 2018[10] that showed a significant decrease in pre- and post- treatment scores of plaque index and gingival index by oil pulling method using coconut oil from baseline to 15th and 30th days. Amith et al. found that oil pulling with sunflower oil significantly reduced plaque and gingival index after 45 days.[1] Furthermore, decrease in plaque induced gingivitis was found in oil pulling therapy with sesame oil, which is as effective as chlorhexidine. Similarly, there was a significant decrease in plaque and gingival index at the end of six weeks.
The limitations of the study were short sample size and short duration (6 weeks) of follow-up. Hence, extensive studies with large samples, varying time periods, and long follow- up times should be carried out to establish the accuracy of oil pulling therapy. Research on oil pulling procedure using different types of oil and their effect on oral hygiene is needed. Furthermore, microbiological analysis of saliva and plaque, if considered, will add more internal validity to such studies. Further, studies comparing the effect of various commonly prescribed mouthwashes and oil pulling on oral hygiene are warranted. To avoid the deleterious effects of chemicals in mouth rinses such as staining, altered taste, allergy, and high cost, it is better to switch to nature for its goodness.
CONCLUSION
From the result obtained it can be concluded that there is a statistically significant reduction in the mean gingival index and mean plaque index of Group A when compared to Group B due to the usage of coconut oil as an adjunct in the oral hygiene practices manifesting the effectiveness of oil pulling on plaque and gingivitis. The purpose of this study was to establish an overview of oil pulling therapy with coconut oil as a usable, safe, and cost-effective agent with minimal side effects that can be used as an adjunct in oral hygiene maintenance.
Acknowledgment
The authors would like to acknowledge the manufacturer of Tendders Wonders Gandoosha Thaila by Tendders Wonders LLP, Chennai, for supplying the coconut oil used for this study. The authors also thanked all the study participants without whom this study will not be conducted.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Effect of oil pulling on plaque and gingivitis. J Oral Health Community Dent. 2007;1:12-8.
- [CrossRef] [Google Scholar]
- Polyherbal formulation: Concept of ayurveda. Pharmacogn Rev. 2014;8:73-80.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of oil pulling with sesame oil on plaque-induced gingivitis: A microbiological study. J Orofac Res. 2013;3:175-80.
- [Google Scholar]
- Oil pulling and importance of traditional medicine in oral health maintenance. Int J Health Sci (Qassim). 2017;11:65-70.
- [Google Scholar]
- Oil pulling for better oral health-myth or reality? J Complement Med Altern Healthc. 2018;6:555693.
- [CrossRef] [Google Scholar]
- Effect of oil pulling in promoting oro dental hygiene: A systematic review of randomized clinical trials. Complement Ther Med. 2016;26:47-54.
- [CrossRef] [PubMed] [Google Scholar]
- Coconut oil pulling-the holistic medicine: Evaluation of efficacy of coconut oil pulling therapy as an adjunct to scaling in diabetic patients with chronic gingivitis-a clinical and microbiological study. J Interdiscip Dent. 2019;9:59-65.
- [CrossRef] [Google Scholar]
- Comparison of a manual and a new electric toothbrush for controlling plaque and gingivitis. J Clin Periodontol. 1994;21:86-90.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of coconut oil pulling on plaque-induced gingivitis: A prospective clinical study. Int J Green Pharm. 2018;11:1355.
- [Google Scholar]




