
Translate this page into:
Efficacy of alveolar sandwich osteotomy with simultaneous implant placement for the management of vertical deficiency

*Corresponding author: Nivedhini Priya Muthu, Department of Oral and Maxillofacial Surgery, Ragas Dental College and Hospital, Chennai, Tamil Nadu, India. drnivedhini@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Muthu NP, Vijayarangan S, Jeyakumar S, Deenadayalan V. Efficacy of alveolar sandwich osteotomy with simultaneous implant placement for the management of vertical deficiency. J Global Oral Health 2023;6:20-5.
Abstract
Objectives:
The aim of this present study was to evaluate the efficacy of the alveolar sandwich osteotomy with simultaneous implant placement for the management of vertical deficiency.
Materials and Methods:
This study was conducted in the Department of Oral and Maxillofacial Surgery, Ragas Dental College, Chennai. A total of 10 partially edentulous patients with reduced alveolar ridge height were selected for the study and sandwich osteotomy with simultaneous implant placement was done. All patients underwent radiographic evaluation preoperatively and postoperatively at 0, 1, and 3 months, respectively.
Results:
Of the 20 implant sites, the pre-operative ridge height varied from a minimum of 6 mm to the maximum of 8 mm with the mean of 7 ± 0.4 mm. The mean length of the alveolar ridge achieved during immediate postoperative period was 10.6 ± 3 mm and at 1st-month post-operative period it was 10.5 ± 3 and at 3-month post-operative period, it was 10.4 ± 3, all patients were followed up for a period of 3-month postoperatively.
Conclusion:
Sandwich osteotomy with simultaneous implant placement can be successfully used in patients with moderate alveolar deficiency to increase alveolar bone height.
Keywords
Sandwich osteotomy
Vertical augmentation
Implants
Piezoelectric surgery

INTRODUCTION
Tooth loss may have a variety of causes such as trauma, periodontal disease, and caries leading to pulpitis. The alveolar bone is a tooth-dependent tissue.[1] The shape and the volume of the alveolar process are influenced by the tooth form, the direction of the eruption of the tooth and the presence or absence of teeth. Thus, loss of teeth invariably leads to atrophy of the residual alveolar ridge in relation to both height and width.[2]
In recent years, dental implants represent a reliable treatment option for restoring oral function in edentulous and partially edentulous patients. Availability of sufficient bone volume is, however, an important prerequisite for the successful insertion of a dental implant, because an insufficient ridge volume will result in incomplete coverage of the implant by bone and a possible recession of the covering soft tissues.[3] Alveolar ridge deficiency has become extremely challenging and is considered a major limitation for successful implant placement, as well as for the long-term success rate.
Vertical augmentation of the alveolar ridge is necessary for patients with extensive resorption of the alveolar ridge to place implants. Numerous augmentation techniques have been proposed to increase bone height in atrophic alveolar ridges. Among these, the sandwich osteotomy is a predictable surgical procedure that can be used to augment vertical alveolar bone. Sandwich osteotomy with the use of an interpositional bone graft was first described by Schettler in 1976 for anterior mandible to improve the retention of a full denture.[4]
MATERIALS AND METHODS
Source of data
This study was conducted at Ragas Dental College and Hospital in the Department of Oral and Maxillofacial Surgery from December 2019 to December 2021. The protocol for this study was accepted by the Institutional Review Board (IRB NO: 20191216) on December 2019.
The study population consisted of 10 apparently healthy patients between 20 and 60 years of age, who are partially edentulous with reduced vertical alveolar ridge height coming for implant treatment.
Partially edentulous patients with vertical dimensions <8 mm and crestal alveolar widths not <5 mm were included in the study. Patients with local pathology, systemic diseases, and medications that may interfere with bone healing and osseointegration were all excluded from the study.
All patients were evaluated as per standard norms, written informed consent was obtained from all the patients. Under strict aseptic precautions, the surgical site was anesthetized. A pyramidal flap was reflected with osteotomy cuts being made using piezotome [Figures 1 and 2]. The implant osteotomy site was prepared to its full length and the alveolar segment was separated from the basal bone with a chisel maintained in its position to the required height [Figures 3 and 4]. The gap was augmented with alloplastic bone particulate and covered with collagen membrane following which the mucoperiosteal flap was advanced and sutured [Figures 5 and 6].
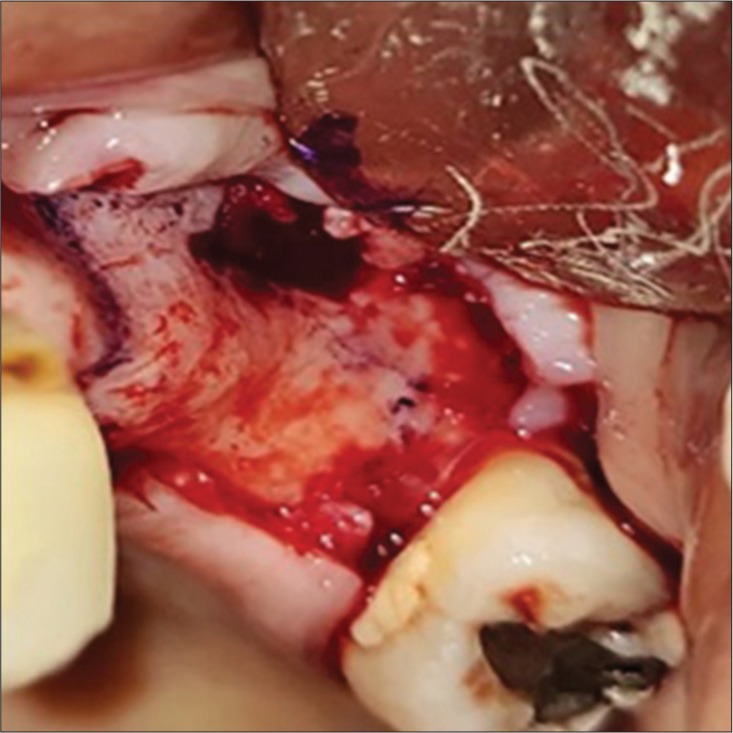
- Labial flap reflected without disturbing the palatal mucosa.
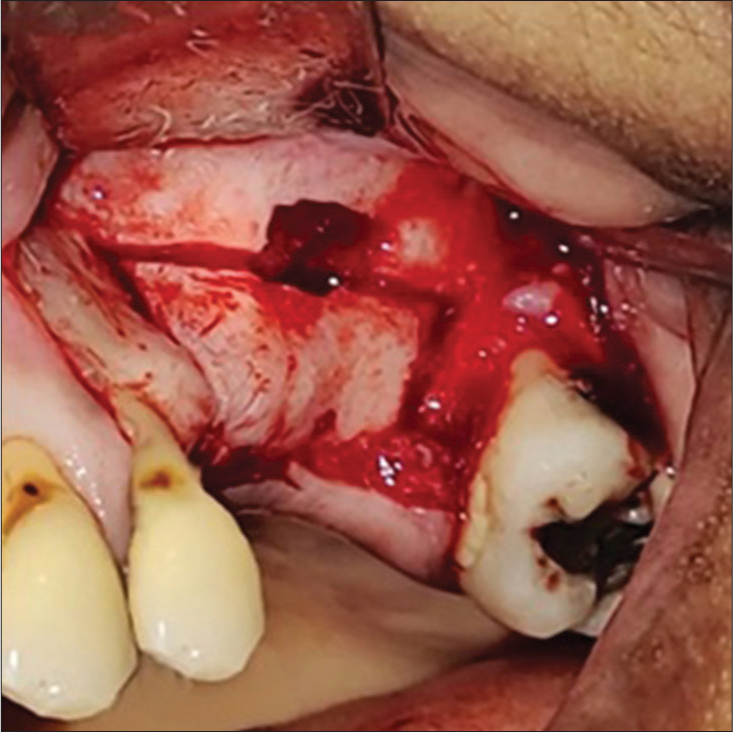
- Two vertical osteotomy cuts connected by a horizontal cut were done using piezotome.

- The alveolar segment was separated from the basal bone using chisel.

- The segment was down fractured and two implants were placed.

- The gap between the transported segment and the basal bone was filled with alloplastic bone particulate.

- The site was sutured with 5-0 ethilon sutures.
RESULTS
The purpose of the study was to evaluate the efficacy of the alveolar sandwich osteotomy with simultaneous implant placement for the management of vertical deficiency. The patients selected in our study primarily had vertical alveolar deficiency without concomitant horizontal alveolar deficiency. A total of ten partially edentulous sites with vertical alveolar deficiency were augmented by sandwich osteotomy and 20 simultaneous implants were placed. All patients underwent radiographic evaluation preoperatively and postoperatively at 0, 1, and 3 months, respectively [Figures 7-10]. The gain in vertical height postoperatively from the baseline was assessed and the data were tested for normality using analysis of variance. The statistical analysis was interpreted with the results obtained by keeping the P = 0.05 as a significance level. Of the 20 implant sites, the pre-operative ridge height varied from a minimum of 6 mm to the maximum of 8 mm with the mean of 7 ± 0.4 mm. The mean length of the alveolar ridge achieved during immediate postoperative period was 10. 6 ± 3 mm and during 1st month post-operative period, it was 10.5 ± 3 and at 3-month post-operative period it was 10.4 ± 3 [Table 1].

- Pre-operative Orthopantomogram.

- Post-operative Orthopantomogram.

- Pre-operative cone-beam computed tomography.

- Post-operative cone-beam computed tomography.
| Sample no. | Tooth no. | Pre-operative ridge height |
Vertical height gain |
Immediate Post-operative ridge height | Post-operative ridge height in 3-month follow-up |
|---|---|---|---|---|---|
| Sample 1 | 25,26 | 25- 6.6 mm | 4.8 mm | 11.4 mm | 11.3 mm |
| 26- 6.5 mm | 4.9 mm | 11.4 mm | 11.2 mm | ||
| Sample 2 | 35,36 | 35- 6.5 mm | 2 mm | 8.5 mm | No follow-up |
| 36- 6 mm | 2.2 mm | 8.2 mm | No follow-up | ||
| Sample 3 | 24,25 | 24- 8.1 mm | 3 mm | 11.1 mm | 10.8 mm |
| 25- 7.8 mm | 3.1 mm | 10.9 mm | 10.7 mm | ||
| Sample 4 | 46,47 | 46- 7.4 mm | 3.1 mm | 10.5 mm | 10.3 mm |
| 47- 7 mm | 3mm | 10 mm | 9.8 mm | ||
| Sample 5 | 41,42 | 41- 7.3 mm | 3.9 mm | 11.2 mm | 11.1 mm |
| 42- 7.5 mm | 4.1 mm | 11.6 mm | 11.3 mm | ||
| Sample 6 | 11,21 | 11- 6.2 mm | 4.3 mm | 10.5 mm | 10.2 mm |
| 21- 6.5 mm | 4.1 mm | 10.6 mm | 10.3 mm | ||
| Sample 7 | 26,27 | 26- 7.3 mm | 4.2 mm | 11.5 mm | 11.3 mm |
| 27- 7.4 mm | 4 mm | 11.4 mm | 11.2 mm | ||
| Sample 8 | 15,16 | 15- 6.8 mm | 3.9 mm | 10.7 mm | 10.6 mm |
| 16- 6.6 mm | 4 mm | 10.6 mm | 10.4 mm | ||
| Sample 9 | 15,16 | 15- 7.3 mm | 4.4 mm | 11.7 mm | 10.5 mm |
| 16- 7.2 mm | 4.3 mm | 11.5 mm | 10 mm | ||
| Sample 10 | 45,46 | 45- 7.9 mm | 3.5 mm | 11.4 mm | 11.2 mm |
| 46- 7.5 mm | 3.7 mm | 11.2 mm | 11.1 mm |
DISCUSSION
Failure to replace the missing teeth not only causes changes in the bony architecture, but also affects the overlying soft tissues of the alveolus. Thus, following extraction of the tooth, usually a rapid resorption takes place in the alveolar bone.[5,6] Approximately, about 40–60% of loss in alveolar bone height and width occurs within 2–3 years, if the dentition is not restored.[7] The lack of sufficient alveolar bone to place the implants becomes a major limitation for the success and the maintenance of long-term stability of the implant. Therefore, various bone augmentation techniques have been proposed till date to increase the vertical height of the alveolar ridge which includes: onlay block grafting, alveolar distraction osteogenesis, guided bone regeneration, and short implants.
Augmentation of vertically atrophic posterior mandibles with onlay bone grafts has been well-documented in the literature. Although the average vertical bone gain will be 4–5 mm, the results have not been promising as it is prone to graft exposure with the rate of up to 40% of unpredictable graft resorption.[8,9] Distraction osteogenesis has a major disadvantage of vector control which often leads to palatal or lingual inclination of the transport segment. Other potential complications include premature consolidation, infection, and resorption of the transported fragment.[10,11] The use of titanium mesh showed evidence of vascular ingrowth into the graft and new bone formation. However, the stiffness of the titanium mesh causes mechanical irritation to the mucosal flaps with the risk of exposure which also need to be removed during the second surgery.[12,13] Short implants are well-known procedure when the alveolar bone height is inadequate for regular implants. They were used to counter the deficient bone but the altered crown implant ratio presented in the esthetic zone with high smile line was unacceptable.
The rationale of the sandwich osteotomy technique is based on the theory that biomaterial sandwiched between the pedicled bone with the outer cortex and internal cancellous bone undergoes rapid and complete healing and the graft incorporation with a lower percentage of resorption.[14] It is most important to keep the lingual periosteum intact during osteotomy to maintain the blood supply to the mobile bone segment which, in turn, reduces crestal bone resorption following the first stage of surgery.[15-17] Any attempt to displace the segment greater than 5 mm not only risk the potential for vascular embarrassment by detaching periosteal blood supply, but also can excessively rotate the segment palatally because of the reduced extensibility of the palatal mucoperiosteum.[18,19] If the osteotomized bone height is < 4 mm, the segmented bone fragment would be thin and is susceptible to fracture which leads to complete failure of the technique.[20] It is also important that the segment should be elevated only to the level of the cementoenamel junction of adjacent teeth.[9] Furthermore, the width of the osteotomized segment should not be narrower than 5 mm. Our inclusion criteria impose that the distal tooth presence is necessary for loading the implants because the absence of distal tooth in the site of sandwich osteotomy makes the cranial segment unstable. A piezoelectric device was used which provides precise osteotomy without damaging the adjacent soft tissues, thus minimizing the risk of injuring the lingual flap and periosteum with minimal loss of bone.[21,22] Periosteal scoring was done to release the elastic fibers to produce laxity and to provide tension-free wound closure.[23] Failure to do so may result in wound dehiscence and eventually the graft exposure or infection.[24] Patients with thick soft-tissue biotypes had good healing index than patients with thin soft-tissue biotypes. In patients with a thick soft-tissue biotype, we noted a prominent tipping of the osteotomized segment either lingually/palatally.[25] From the shorter duration of observation, all the placed implants were stable. We were limited to the fact that the patients were reviewed for a shorter duration of time. Furthermore, we would like to follow up on all the patients after the secondary loading of the implants for 10 years.
CONCLUSION
Thus, we conclude that sandwich osteotomy with simultaneous implant placement can be successfully used in patients with moderate alveolar deficiency. However, additional randomized, controlled, and clinical trials with long-term observation are needed to test the efficacy of the investigated technique, identify the grafting material of choice, assess the vertical stability of the augmented alveolar ridge, and document the long-term success rate of the dental implants.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
References
- Reduction of residual ridges: A major oral disease entity. J Prosthet Dent. 1971;26:266-79.
- [CrossRef] [PubMed] [Google Scholar]
- Vertical ridge augmentation using a membrane technique associated with osseointegrated implants. Int J Periodontics Restorative Dent. 1994;14:496-511.
- [Google Scholar]
- Sandwich-technique with cartilage transplant for raising the alveolar process in the lower jaw. Fortschr Kiefer GesichtsChir. 1976;20:61-3.
- [Google Scholar]
- Bone healing and soft tissue contour changes following single-tooth extraction: A clinical and radiographic 12-month prospective study. Int J Periodontics Restorative Dent. 2003;23:313-23.
- [Google Scholar]
- Alveolar bone dimensional changes of post-extraction sockets in humans: A systematic review. J Clin Periodontol. 2009;36:1048-58.
- [CrossRef] [PubMed] [Google Scholar]
- Postextraction ridge preservation using a synthetic alloplast. Implant Dent. 2000;9:168-76.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical results of alveolar ridge augmentation with mandibular block bone grafts in partially edentulous patients prior to implant placement. Clin Oral Implants Res. 2002;13:103-11.
- [CrossRef] [PubMed] [Google Scholar]
- Alveolar sandwich osteotomy in resorbed alveolar ridge for dental implants: A 4-year prospective study. J Oral Maxillofac Surg. 2014;72:292-303.
- [CrossRef] [PubMed] [Google Scholar]
- Analysis of complications following alveolar distraction osteogenesis and implant placement in the partially edentulous mandible. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;100:25-30.
- [CrossRef] [PubMed] [Google Scholar]
- Complications in alveolar distraction osteogenesis of the atrophic mandible. Int J Oral Maxillofac Surg. 2007;36:916-21.
- [CrossRef] [PubMed] [Google Scholar]
- The use of titanium mesh in guided bone regeneration: A systematic review. Int J Dent. 2019;2019:9065423.
- [CrossRef] [PubMed] [Google Scholar]
- Prosthetically CAD-CAM-guided bone augmentation of atrophic jaws using customized titanium mesh: Preliminary results of an open prospective study. J Oral Implantol. 2018;44:131-7.
- [CrossRef] [PubMed] [Google Scholar]
- Vertical ridge augmentation of the atrophic posterior mandible with sandwich technique: Bone block from the chin area versus corticocancellous bone block allograft--clinical and histological prospective randomized controlled study. Biomed Res Int. 2014;2014:982104.
- [CrossRef] [PubMed] [Google Scholar]
- Biologic basis for interpositional autogenous bone grafts to the mandible. J Oral Maxillofac Surg. 1982;40:407-11.
- [CrossRef] [PubMed] [Google Scholar]
- Sandwich osteotomy for vertical and transversal augmentation of the posterior mandible. Int J Oral Maxillofac Surg. 2010;39:554-60.
- [CrossRef] [PubMed] [Google Scholar]
- Segmental sandwich osteotomy of the posterior mandible in pre-implant surgery-A systematic review. Med Oral Patol Oral Cir Bucal. 2017;22:e132-41.
- [CrossRef] [PubMed] [Google Scholar]
- Alveolar segmental sandwich osteotomy for anterior maxillary vertical augmentation prior to implant placement. J Oral Maxillofac Surg. 2006;64:290-6. Erratum in: J Oral Maxillofac Surg 2006;64:997
- [CrossRef] [PubMed] [Google Scholar]
- Interpositional osteotomy for posterior mandible ridge augmentation. J Oral Maxillofac Surg. 2009;67:31-9.
- [CrossRef] [PubMed] [Google Scholar]
- Vertical ridge augmentation of the atrophic posterior mandible with interpositional bloc grafts: Bone from the iliac crest vs. bovine anorganic bone. Clinical and histological results up to one year after loading from a randomized-controlled clinical trial. Clin Oral Implants Res. 2009;20:1386-93.
- [CrossRef] [PubMed] [Google Scholar]
- The piezoelectric bony window osteotomy and sinus membrane elevation: Introduction of a new technique for simplification of the sinus augmentation procedure. Int J Periodontics Restorative Dent. 2001;21:561-7.
- [Google Scholar]
- Piezoelectric vertical bone augmentation using the sandwich technique in an atrophic mandible and histomorphometric analysis of mineral allografts: A case report series. Int J Periodontics Restorative Dent. 2010;30:383-91.
- [Google Scholar]
- "PASS" principles for predictable bone regeneration. Implant Dent. 2006;15:8-17.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of absorbable membranes on sandwich bone augmentation. Clin Oral Implants Res. 2008;19:32-41.
- [Google Scholar]
- Palatal approach to the anterior maxillary sandwich osteotomy. J Oral Maxillofac Surg. 2013;71:1005-9.
- [CrossRef] [PubMed] [Google Scholar]




