
Translate this page into:
Factors affecting “preparedness for practice” among newly graduated dentists – A cross-sectional study

*Corresponding author: Malu Mohan, Public Health Research Consultant, Women’s Institute for Social and Health Studies, AGRA - 32, Anayara, Thiruvananthapuram - 695029, Kerala, India. dr.malumohan@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Mohan M, Ravindran TKS. Factors affecting “preparedness for practice” among newly graduated dentists – A cross- sectional study. J Global Oral Health 2020;3(1):23-33.
Abstract
Objectives:
Consequent to the drastic growth that has occurred over the past few decades in the dental education sector, dental profession in India, has also undergone changes. Hence, it is critical to inquire whether the current training that is being offered to dental students is successful in preparing them adequately to meet the challenges of the changing dental profession. We have aimed to assess the level of preparedness for independent dental practice among newly graduated dentists of Kerala and to explore the factors associated with their preparedness.
Materials and Methods:
This cross-sectional survey was conducted among a random sample of 400 recently graduated dentists from Kerala. We developed and validated a self-administered scale named Preparedness for Practice among Dental Graduates-Scale, PPDG-S, to assess the level of preparedness. The overall preparedness scores were categorized based on the median value of the total score (87) – score less than or equal to the median was considered “low preparedness” (0–87) and score greater than the median (>87) was considered “high preparedness.” The difference in proportion between high and low prepared participants across socio- demographic background, training characteristics, and employment characteristics was assessed and the significance was tested using the Chi-square test. A binary logistic regression analysis was conducted to identify the predictors of preparedness among recent dental graduates.
Results:
The majority of the participants reported themselves to be in the “low preparedness” category (209, 52.3%) as compared to the “high preparedness” category (191, 47.8%). In the bivariate analysis, five variables were found to have significant differences in their proportions between the high and low preparedness categories – gender, caste, type of training institution, work experience, and frequent job changes. According to multivariate analysis, being trained in a private/cooperative college (as opposed to a public institution) and not possessing continuous work experience of even 1 year in a single job (as opposed to having a continuous work experience) were found to pose significant adjusted risk for the lower preparedness among graduates.
Conclusion:
The high proportion of our study participants reporting lower preparedness for independent practice, reflect poor self-rating of their employability. This is critical, when we consider the competitive, saturated private practice sector, and unemployment among young dentists. The relatively higher proportion of poor preparedness among the private sector trained graduates when compared to the government college trained graduates is another matter that raises concern.
Keywords
Preparedness for practice
Dental graduates
Dental profession
Dental education
Dental training
Employability

INTRODUCTION
Dental profession in India has undergone significant changes over the past few decades consequent to the drastic growth which has occurred in the dental education sector. The rising presence of private sector in health professional education has been criticized by many quarters in academia over the past three decades. The critics of rampant privatization have repeatedly raised the issue of inadequate exposure of private college trained students to clinical material, due to lesser patients visiting these institutions.[1-3] The situation appears even graver, when its consequences are reflected in the context of the poorly monitored and increasingly saturated private dental practice sector, especially in urban India.
Dental care is almost exclusively delivered in the private sector in India and <5% dentists’ practice in the public sector. There have been reports of unfavorable professional circumstances like unemployment among dental graduates from across the world and India.[4-6] A recently published cross-sectional survey in Kerala, reports the presence of high unemployment and financial vulnerability among freshly graduated dental practitioners. The highly crowded and competitive private practice sector remains the predominant employment avenue for the dental graduates in the state. One major observation made by the study was that the public sector trained graduates fared considerably better than private sector graduates in terms of securing employment and receiving a decent remuneration.[7]
Under these circumstances, it is critical to enquire whether the current training which is being offered to dental students is successful in preparing them adequately to meet the changing dental profession. The findings of such an inquiry will reflect not only on the extent to which dental training has prepared them, but also on the potential quality of dental care delivered. “Preparedness for practice” is a concept different from other similar concepts which have been used in the literature to explore the quality of health professions, such as competencies or Entrustable Professional Activities. These concepts reflect the extent to which new graduates or learners have imbibed the knowledge and skills required for independent practice, imparted to them through the training process. However, they do not consider the extent to which the graduates are prepared to work independently in the prospective or new settings of employment and cope with the potentially diverse and complex challenges awaiting them. We have thus conceptualized “preparedness” as a concept that encompasses the knowledge, skills, and other professional attributes that will prepare a new graduate to transition from being an intern or resident in the ideal and/or familiar settings of their training institution, to an independent professional, ready for a less than ideal, and messy and/or unfamiliar work place.[8] In other words, we have conceptualized “preparedness” as a measure of employability. Through this study, we have aimed to assess the level of preparedness for independent dental practice among newly graduated dentists of Kerala and to explore the factors associated with preparedness.
MATERIALS AND METHODS
This cross-sectional survey was conducted among a random sample of recently graduated dentists from Kerala. The sample size was statistically determined at 95% confidence interval and an absolute precision of 5%, a non-response rate of 9%, the sample size was estimated to be 399 (rounded off to 400).[9] All registered dental graduates who completed BDS degree between 2014 April and 2018 February from any recognized (by the Dental Council of India) public or private dental college within Kerala, with permanent address (as per the information provided at the State Dental Council) in one of the six districts of south and central Kerala (Thiruvananthapuram, Kollam, Alappuzha, Pathanamthitta, Kottayam, and Ernakulam) were included in the study.
Circular systematic random sampling was employed, in which, the total number of graduates in each district is divided by the number of graduates required in each category (public or private), to obtain the sampling interval in each category. The sample was selected such that the district-wise ratios of graduates in the sampling frame were maintained. The sample from each district also maintained the public- trained to private-trained ratios of the sampling frame from the corresponding district.
The Institutional Ethics Committee cleared the proposal for the study, during July 2017 (SCT/IEC/1069/June-2017). Written informed consent was sought from every participant.
Study tools
A self-administered survey pro forma collecting information about the basic socio-demographic profile, employment options, and career choices of recent graduates was used among the participants. Following this, we did an assessment of preparedness for independent practice among recent graduates using the 30-item scale (Preparedness for Practice among Dental Graduates-Scale, PPDG-S), which was also self-administered. The scale was scored on a 5-point Likert scale – completely prepared, well prepared, neither well prepared nor poorly prepared, poorly prepared, and completely unprepared).
PPDG-S was developed and validated by the authors for the purpose of this study. It was based on a conceptual framework developed through a combination of meta-synthesis of the literature and qualitative exploration through in-depth interviews with a diverse theoretical sample of community members (age, gender, socio-economic status, and location of residence) and dental professionals (practitioners with different range of experience in clinical practice, dental academicians, and students). The detailed methodology of the meta-synthesis is published elsewhere.[1] The question which was explored during the qualitative exploration was, “what are the attributes that you expect in a dental professional prepared for practice?” An initial item pool was created which was subsequently reduced to an item pool using Exploratory Factor Analysis using Principal Component Analysis Method. Subsequently, we assessed the psychometric properties of the tool.
Statistical analysis
The level of preparedness was assessed using the sum of scores of individual items. We converted the overall preparedness scores into two categories based on the median value of the total score (87) – score less than or equal to the median was considered “low preparedness” (0–87) and score greater than the median (>87) was considered “high preparedness.” The self-reported preparedness of the graduates in the individual items was assessed on the basis of median preparedness scores.
The difference in proportion between high and low prepared participants across socio-demographic background, training characteristics, and employment characteristics was assessed and the significance was tested using the Chi-square test. The multicollinearity of the factors which emerged significant in the bivariate analysis was assessed in a correlation matrix using the variation inflation factor (VIF), and the variables which had the least collinearity when assessed in pairs (VIF value less than the selected arbitrary cutoff value of 5) were used in multivariate analysis.
RESULTS
Psychometric properties of the PPDG-S
The conceptual framework based on which PPDG-S was developed had seven domains [Figure 1]. The scale good internal consistency (Cronbach’s α = 0.935), split half reliability (first half of 15 items, α = 0.908 and second half of 15 items, α= 0.903; r = 0.764) and test-re-test reliability (Pearson’s correlation coefficient, r = 0.945). All 30 items attained the critical content validity ratio value of 0.75 recommended by the Lawshe method of content validity assessment, and the content validity index of the tool was 0.825. The overall agreement among the panellists was estimated using online multi-rater Kappa calculator, and it showed good inter-rater agreement (r = 0.86).[10] The scale was found to have adequate face validity when tested with a purposive sample of 15 fresh graduates and interns. The construct validity of the final 30 item scale of PPDG-S was demonstrated using the rotated component matrix in Exploratory Factor Analysis. It showed good convergent and discriminant validity (final scale attached as supplementary material).
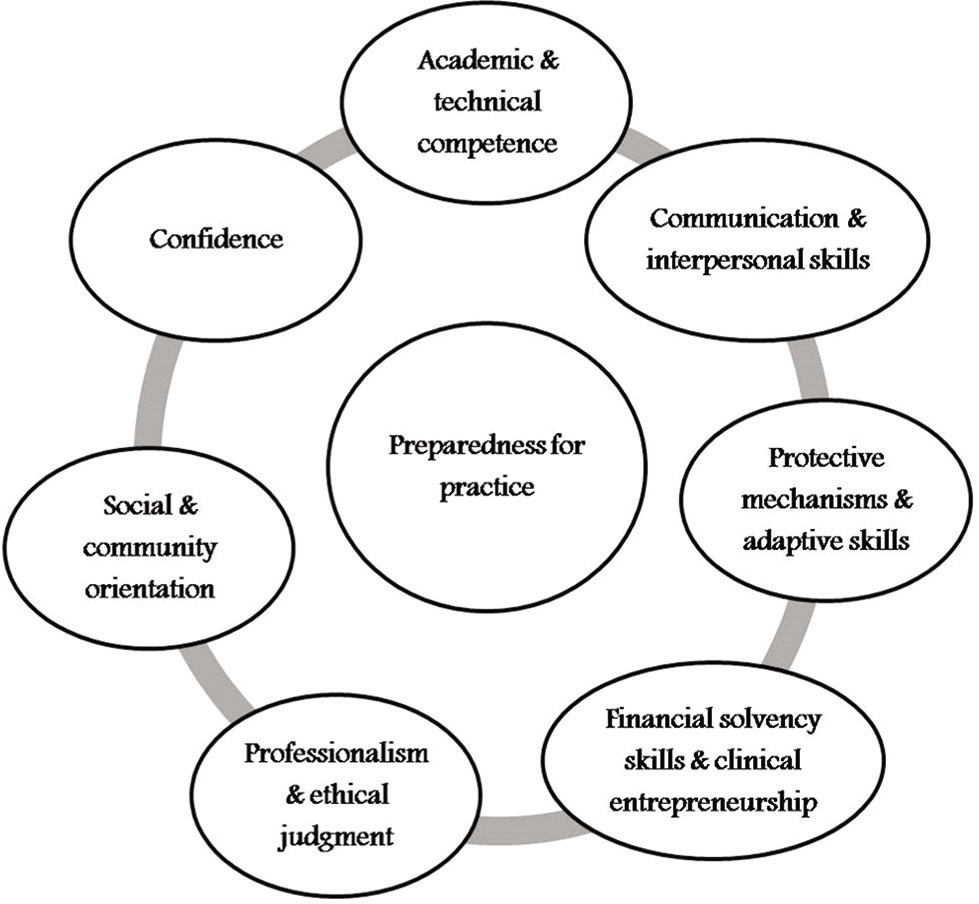
- Conceptual framework explaining “preparedness for practice.”
Profile of the study participants
The detailed socio-demographic profile, training, and employment characteristics of the study sample have been published previously.[7] [Table 1] depicts the overall profile of the study participants. Our study sample was consistent with the gender distribution of the sampling frame with a greater proportion of women. Graduates trained from private dental colleges formed the majority. A greater proportion of graduates gained admission through management/NRI seats rather than through merit. Only a small proportion of the study participants belonged to the Scheduled Castes. A notable proportion of recent dentists in the study sample included either currently unemployed graduates or those who did not earn an income from dentistry.
| Variables | Proportion of participants (%) | |
|---|---|---|
| Gender | Women | 276 (69) |
| Men | 124 (31) | |
| Caste | OBC (non-creamy layer)# | 138 (34.5) |
| General | 132 (32.75) | |
| OBC (creamy layer)## | 97 (24.25) | |
| SC | 33 (8.5) | |
| Number of earning members (Two-income vs. one-income households) | Households with a single source of income (either father or mother) | 298 (74.5) |
| Households with dual sources of income (both father and mother are earning) | 102 (25.5) | |
| Source of financing for graduate education | Financed by parents or family | 187 (46.8) |
| Sale of assets alone | 160 (40) | |
| Educational loan alone | 32 (8.0) | |
| Both of the above | 21 (5.2) | |
| Education: Type of institution | Private | 307 (76.8) |
| Public | 76 (19) | |
| Cooperative | 17 (4.3) | |
| Type of admission to BDS | Management/NRI | 231 (57.8) |
| Merit | 169 (42.2) | |
| Employment status | Currently employed* in dentistry with an income | 269 (67.3) |
| Currently employed* in dentistry without an income | 19 (4.7) | |
| Currently not employed* in dentistry | 112 (28.0) | |
# - The members of the Other Backward Communities caste category who are eligible for the 27% reservation in education and jobs as per the directions of the Ministry of Human Resource Development, since the income level of their families’ is less than six lakhs per annum; ## - the members of the Other Backward Communities caste category who are not eligible for the 27% reservation in education and jobs since they are considered “socially advanced” as per the directions of the Ministry of Human Resource Development, since the income level of their families’ is more than 6 lakhs per annum.
Preparedness for practice among study participants
Through Figures 2 and 3, we describe the distribution of preparedness scores. The mean score was 85.26 out of a maximum attainable score of 120. The normality of the distribution was assessed using Shapiro–Wilk test, and it was found to be significant confirming a non-normal distribution (Shapiro–Wilk statistic – 0.968, P = 0.000).
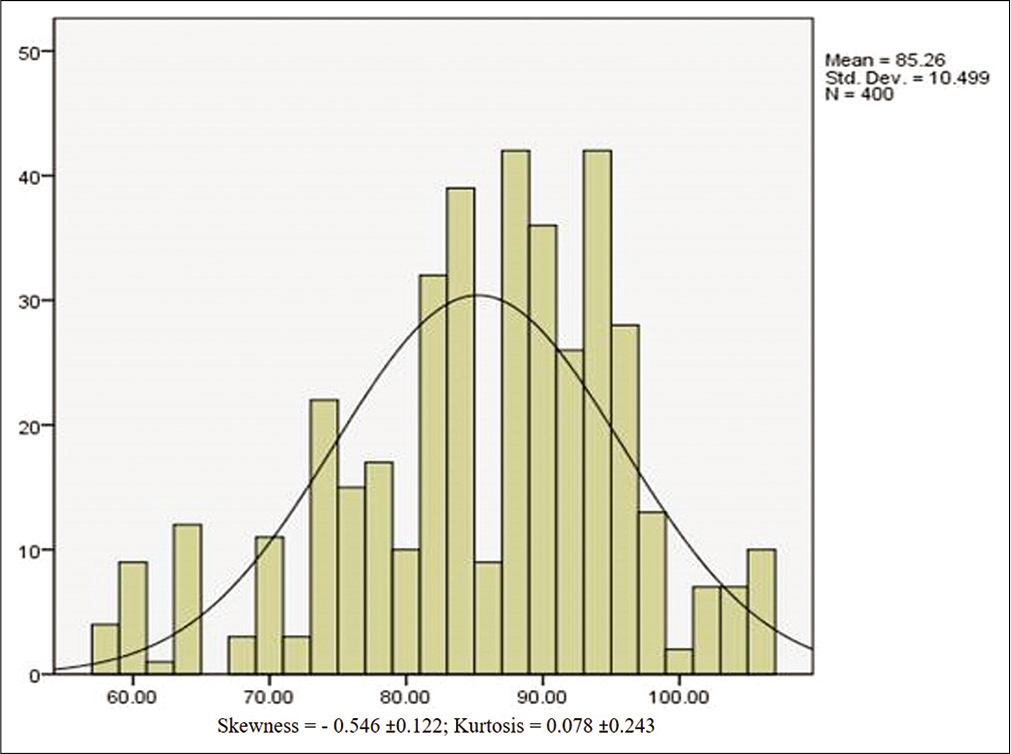
- Histogram with a normality plot.
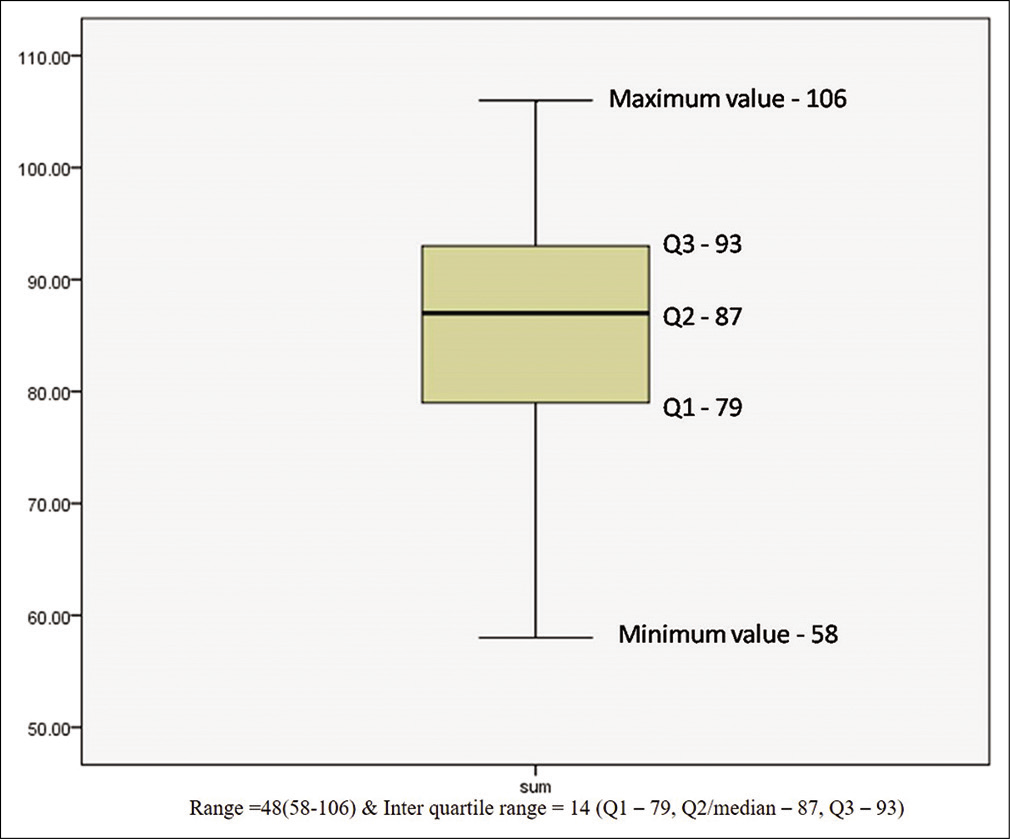
- Box plot describing the data distribution of total preparedness scores.
The majority of the participants reported themselves to be in the “low preparedness” category (209, 52.3%) as compared to the “high preparedness” category (191, 47.8%). The graduates generally felt “well prepared” or “completely prepared” in 26 of the 30 areas considered by the scale across five domains, namely – competence in general oral health assessment and preventive care (items 1–4), technical competence in clinical care (items 5–13), independent management of dental practice (items 14–20), communication and interpersonal skills (items 21–26), and patient-centered dental practice (items 27–30). The median scores reflect that they generally felt ambivalent (“neither prepared nor unprepared”) in four areas – orthodontic treatment planning (item 9 under technical competence in clinical care), confidence to independently manage emergency situations in dental office (item 14 under independent management of dental practice), confidence in one’s ability to independently run a profitable dental clinic (item 16 under independent management of dental practice), and setting up of an independent dental practice in Kerala (item 17 under independent management of dental practice). In [Table 2], we have combined the scores of each item and dichotomized them into prepared (combined well prepared and completely prepared) and poorly prepared (combined completely unprepared, poorly prepared and neither prepared nor unprepared).
| Domain/Item | High preparedness | Low preparedness |
|---|---|---|
| Competence in general oral health assessment and preventive care (%) | ||
| Diagnosis | 314 (78.5) | 86 (21.5) |
| Treatment plan | 377 (94.25) | 23 (5.75) |
| Non-surgical management of periodontal problem | 320 (80) | 80 (20) |
| Preventive care | 352 (88) | 48 (12) |
| Technical competence in clinical care (%) | ||
| Conservative restorative care | 366 (91.5) | 34 (8.5) |
| Aesthetic restorative care | 299 (74.75) | 101 (25.25) |
| Crowns | 213 (53.25) | 187 (46.75) |
| Dentures | 297 (74.25) | 103 (25.75) |
| Orthodontic treatment planning | 124 (31) | 276 (69) |
| Local anesthesia | 204 (51) | 196 (49) |
| Oral surgical procedures | 336 (84) | 64 (16) |
| Endodontic treatment | 221 (55.25) | 179 (44.75) |
| Drug prescription | 314 (78.5) | 86 (21.5) |
| Independent management of dental practice (%) | ||
| Emergency situations | 163 (40.75) | 237 (59.25) |
| Independent patient management | 299 (74.75) | 101 (25.25) |
| Profitabledental clinic | 186 (46.5) | 214 (53.5) |
| Set up of dental clinic | 153 (38.25) | 247 (61.75) |
| Work place hazards | 238 (59.5) | 162 (40.5) |
| Iatrogenic problems | 299 (74.75) | 101 (25.25) |
| Creation of learning opportunities | 210 (52.5) | 190 (47.5) |
| Communication and Interpersonal skills (%) | ||
| Patient communication | 250 (62.5) | 150 (37.5) |
| Sensitive information | 289 (72.25) | 111 (27.75) |
| Communication with support staff | 374 (93.5) | 26 (6.5) |
| Management of fearful patients | 300 (75.0) | 100 (25.0) |
| Patients with special needs | 210 (52.5) | 190 (47.5) |
| Shared decision making | 356 (89.0) | 44 (11.0) |
| Patient centered dental care (%) | ||
| Informed consent | 333 (83.25) | 67 (16.75) |
| Confidentiality | 331 (82.75) | 69 (17.25) |
| Privacy | 379 (94.75) | 21 (5.25) |
| Consideration of patient compliance | 350 (87.5) | 50 (12.5) |
In the bivariate analysis, five variables were found to have significant differences in their proportions between the high and low preparedness categories – gender, caste, type of training institution, work experience, and frequent job changes [Table 3]. A greater proportion of women reported high preparedness as compared to men (51.4% as opposed to 39.5%). A significantly higher proportion of graduates from SC category reported low preparedness (87.9%) compared to the other categories. A greater proportion of graduates who trained in government dental colleges (63.2%) reported high preparedness than the graduates who trained in private or cooperative colleges (44.1%). However, the type of channel through which the candidate secured admission in a college – merit quota or management/NRI quota – did not seem to influence the differential proportion of graduates.
| Factors | Low preparedness (n=209) | High preparedness (n=191) | Chi-square | P-value |
|---|---|---|---|---|
| Socio-demographic background (%) | ||||
| Gender | 4.883 | 0.027 | ||
| Men (n=124) | 75 (60.5) | 49 (39.5) | ||
| Women (n=276) | 134 (48.6) | 142 (51.4) | ||
| Caste | 25.545 | 0.000 | ||
| SC (n=33) | 29 (87.9) | 4 (12.1) | ||
| OBC (non-creamy layer) (n=138)# | 56 (40.6) | 82 (59.4) | ||
| OBC (creamy layer) (n=97)## | 49 (50.5) | 48 (49.5) | ||
| General (n=132) | 75 (56.8) | 57 (43.2) | ||
| Training background | ||||
| Type of institution | 8.928 | 0.003 | ||
| Public (n=76) | 28 (36.8) | 48 (63.2) | ||
| Private/cooperative (n=324) | 181 (55.9) | 143 (44.1) | ||
| Type of seat | 0.118 | 0.731 | ||
| Merit seat (n=169) | 90 (53.3) | 79 (46.7) | ||
| Management/NRI seats (n=231) | 119 (51.5) | 112 (48.5) | ||
| Work experience | ||||
| Current employment status | ||||
| Unemployed (n=108) | 74 (66.1) | 38 (33.9) | 11.911 | 0.001 |
| Employed (n=288) | 135 (46.9) | 153 (53.1) | ||
| Past employment status | ||||
| Unemployed in the past (n=68) | 12 (17.6) | 56 (82.4) | 39.319 | 0.000 |
| Employed in the past (n=332) | 197 (59.3) | 135 (40.7) | ||
| <1 year (n=95)* | 79 (83.2) | 16 (16.8) | 53.469 | 0.000 |
| <24 months (n=182) | 84 (46.2) | 98 (53.8) | ||
| 24–48 months (n=118) | 41 (34.7) | 77 (65.3) | ||
| Number of job changes till now (n=395)** | ||||
| Changed jobs <3 times (n=248) | 104 (41.9) | 144 (58.1) | 32.222 | 0.000 |
| Changed jobs 3 times or more times (n=147) | 105 (1.4) | 24 (28.6) |
All the variables considered under the work experience of graduates were found to be associated with the overall preparedness for practice. Among the highly prepared, the proportion of the currently employed (53.1%) and those employed in the past (59.3%) were much higher than the proportion of currently unemployed (33.9%) and those unemployed in the past (17.6%). The mean number of job changes was found to be inversely correlated with preparedness outcomes, i.e., greater mean number of job changes lower the preparedness. The duration after graduation completion was found to be positively correlated with preparedness outcomes, i.e., greater time elapsed after graduation higher the preparedness. A higher proportion of graduates who spent at least 1 year in the same job (65.8%) reported better preparedness compared to those who spent <1 year in a job (16.8%). The proportion of highly prepared among those who frequently changed jobs (3 or more times since graduation) was significantly lower (28.6%) than those who had greater stability in employment (changed jobs <3 times).
The differences in preparedness based on gender, caste, work experience, and job changes across individual items in the scale are presented in [Table 4].
| Domain/Item | Women (n=276) | Men (n=124) | Belong to SC community (n=33) | Do not belong to SC community (n=367) | Public (n=76) | Private (n=307) | Cooperative (n=17) | Employed continuously in a single job for at least 1 year after graduation (n=300) | Not employed continuously in a singlejob for even 1 year aftergraduation (n=95) |
|---|---|---|---|---|---|---|---|---|---|
| Competence in general oral health assessment and preventive care | |||||||||
| Diagnosis | 191.79 | 219.89 | 176.80 | 202.63 | 240.66 | 187.42 | 257.21 | 201.07 | 189.64 |
| Treatment plan | 188.37 | 227.50 | 195.88 | 200.92 | 236.63 | 189.10 | 244.94 | 207.03 | 194.69 |
| Non-surgical management of periodontal problem | 204.39 | 191.85 | 174.55 | 202.83 | 170.40 | 208.31 | 194.00 | 206.35 | 175.22 |
| Preventive care | 208.50 | 182.69 | 153.97 | 204.68 | 236.05 | 194.11 | 156.94 | 218.51 | 142.09 |
| Technical competence in clinical care | |||||||||
| Conservative restorative care | 226.10 | 143.52 | 153.70 | 204.71 | 198.38 | 204.43 | 138.94 | 221.64 | 133.55 |
| Esthetic restorative care | 210.44 | 178.37 | 164.41 | 203.71 | 223.26 | 192.26 | 247.53 | 212.17 | 159.38 |
| Crowns | 198.19 | 205.64 | 170.83 | 203.17 | 251.36 | 189.58 | 170.26 | 219.89 | 138.32 |
| Dentures | 202.25 | 196.61 | 192.29 | 201.24 | 218.73 | 198.63 | 152.79 | 204.01 | 181.63 |
| Orthodontic treatment planning | 191.40 | 220.76 | 207.26 | 199.89 | 239.21 | 188.25 | 248.65 | 210.10 | 193.56 |
| Local anesthesia | 197.03 | 208.23 | 169.83 | 203.26 | 257.87 | 185.59 | 213.26 | 199.90 | 192.83 |
| Oral surgical procedures | 202.35 | 196.38 | 183.53 | 202.03 | 226.33 | 192.44 | 230.53 | 204.87 | 179.26 |
| Endodontic treatment | 197.00 | 208.29 | 171.14 | 203.14 | 258.59 | 184.07 | 237.59 | 209.86 | 165.67 |
| Drug prescription | 219.45 | 158.33 | 168.38 | 203.39 | 174.71 | 210.28 | 139.26 | 223.48 | 128.52 |
| Independent management of dental practice | |||||||||
| Emergency situations | 197.73 | 206.66 | 187.92 | 201.63 | 271.51 | 180.36 | 246.65 | 208.37 | 169.72 |
| Independent patient management | 203.11 | 194.69 | 140.03 | 205.94 | 224.94 | 195.78 | 196.44 | 213.70 | 155.19 |
| Profitabledental clinic | 196.38 | 209.68 | 195.71 | 200.93 | 281.76 | 178.66 | 231.66 | 211.24 | 161.90 |
| Set up of dental clinic | 200.33 | 200.88 | 179.33 | 202.40 | 249.14 | 186.98 | 227.76 | 203.52 | 195.97 |
| Work place hazards | 175.40 | 256.38 | 212.39 | 199.43 | 265.78 | 183.96 | 207.29 | 194.36 | 207.92 |
| Iatrogenic problems | 180.42 | 245.19 | 206.68 | 199.94 | 251.17 | 187.45 | 209.68 | 195.52 | 204.75 |
| Creation of learning opportunities | 213.29 | 172.04 | 183.89 | 201.99 | 254.31 | 188.52 | 176.29 | 224.04 | 127.01 |
| Communication and interpersonal skills | |||||||||
| Patient communication | 205.81 | 188.69 | 175.00 | 212.79 | 216.47 | 196.90 | 194.09 | 210.72 | 163.31 |
| Sensitive information | 218.23 | 161.04 | 191.58 | 201.30 | 184.47 | 206.67 | 160.68 | 212.19 | 159.33 |
| Communication with support staff | 219.39 | 158.45 | 153.67 | 204.71 | 164.05 | 209.58 | 199.41 | 224.44 | 125.92 |
| Management of fearful patients | 219.26 | 158.73 | 149.61 | 205.08 | 196.88 | 204.25 | 148.97 | 221.90 | 132.85 |
| Patients with special needs | 218.36 | 160.76 | 145.73 | 205.43 | 217.24 | 199.05 | 153.76 | 232.70 | 103.40 |
| Shared decision making | 215.03 | 168.17 | 151.98 | 204.86 | 209.16 | 198.47 | 198.41 | 217.24 | 145.55 |
| Patient-centered dental care | |||||||||
| Informed consent | 223.99 | 148.21 | 155.20 | 204.57 | 192.93 | 202.77 | 193.26 | 220.59 | 136.42 |
| Confidentiality | 196.60 | 209.19 | 171.26 | 203.13 | 239.22 | 192.12 | 178.68 | 216.42 | 147.77 |
| Privacy | 206.99 | 186.05 | 153.56 | 204.72 | 220.20 | 197.04 | 174.88 | 222.17 | 132.10 |
| Consideration of patient compliance | 215.98 | 166.05 | 168.58 | 203.37 | 197.24 | 202.57 | 177.76 | 222.00 | 132.56 |
Men scored significantly higher in general oral health assessment skills such as diagnosis, development of treatment plan, orthodontic treatment planning, and in the management of workplace hazards. Women fared well in conservative and esthetic restorative care, drug prescription, lifelong learning, communication and interpersonal skills, and provision of patient-centered dental care.
The graduates belonging to SC category felt poorly prepared than those belonging to the other caste categories in many areas such as provision of preventive care, in conservative restorative care, in independent patient management, in many areas of communication, and interpersonal skills and patient-centered dental care.
Those who were trained in the public sector training institutions fared consistently better than those who trained in private/cooperative sector institutions in all domains. A greater proportion of those who had been employed continuously in a single job for at least 1 year was better prepared in the domains of technical competence in clinical care, communication, and interpersonal skills and provision of patient-centered care.
Caste was found to be significantly associated with overall preparedness and being an SC graduate posing a high risk for low preparedness in bivariate analysis (unadjusted OR – 12.567). However, due to the low precision of the OR (wide confidence interval) and the relatively smaller proportion of graduates belonging to the category in the sample (n = 33, 8.5%), we did not include caste as a variable in the binary logistic regression mode [Table 5].
| Variables | Unadjusted OR | Adjusted OR | P-value | 95% CI | |
|---|---|---|---|---|---|
| Lower bound | Upper bound | ||||
| Being a male graduate | 1.622 | 1.188 | 0.537 | 0.689 | 2.048 |
| Trained in a private/cooperative college | 2.170 | 2.358 | 0.006 | 1.284 | 4.333 |
| Do not possess a continuous work experience of even 1 year in a single job | 6.913 | 7.406 | 0.000 | 3.182 | 17.235 |
| Change in jobs thrice or more | 3.462 | 1.285 | 0.419 | 0.699 | 2.360 |
OR: Odds ratio, CI: Confidence interval
Gender (being a male graduate as opposed to being a woman) did not predict the risk of low preparedness according to the adjusted OR (the value reduced and was non-significant). The frequency of change of jobs (as opposed to changing jobs <3 times) also did not pose a significant risk. The two factors which posed significant risk to the lower preparedness were – being trained in a private/cooperative college (as opposed to a public institution) and not possessing continuous work experience of even 1 year in a single job (as opposed to having a continuous work experience). The adjusted risk of both these factors was found to be higher than the crude risk, and it was found to be significant.
DISCUSSION
The scale (PPDG-S) used in this study was starkly different from other tools already reported in the literature to assess preparedness for practice. The major difference was in the nature of domains involved in the construct. Competence constitutes the most prominent domain in all of the existing scales and questionnaires. In our scale, however, its representation was proportionate to the other six domains. The incorporation of the perspectives of a diverse group of dental professionals and community members in the development of the construct of preparedness has contributed to this difference
In our survey, in many of the routine procedures involved in basic oral surgical and restorative care, the median scores reflected that the graduates were “well prepared.” The majority of the international studies among recent graduates have also reported high preparedness in most of the routine or “bread and butter” aspects of dental care including general patient management, conservative dentistry, and basic surgical care.[11-13] However, literature from higher education suggests that social desirability has a significant influence on self- reported student outcomes from surveys, especially among undergraduate students.[14-16]
Establishing and managing an independent clinical practice was an area of low preparedness in our study, which was also reported from many studies in the international literature. The poor preparedness in this domain was variedly expressed in the literature as the need for supervision during independent work, preference to secure a job in an established practice soon after graduation over independent practice and a greater confidence among the graduates in their abilities to work in a team of established practitioners rather than independently.[9,17]
Our study found that a combination of three factors, namely – the individual and socio-demographic characteristics (gender, and caste) of the graduate; his or her training experience (the type of training institution attended); and the nature of work circumstance and experiences which await him or her (employment status, possession of continuous work experience, and the number of job changes) – influenced the extent of preparedness of a dental graduate in Kerala.
The multivariate analysis showed that not possessing continuous work experience of at least 1 year after graduation posed a significant risk to be in the low preparedness category. Literature suggests that the opportunity to be mentored after graduation and the nature of work experience were significant factors influencing preparedness for independent practice. The need for opportunities to learn at the workplace was also reiterated in the literature from the fact that majority of the dental graduates preferred joining for paid jobs in dentistry rather than independent practice immediately after graduation.[9]
An experience of “reality shock” was reported in literature among health professional graduates, as a lack of connection between theory and practice, when they initiated independent work.[18-21] This experience of disconnect could explain the poor preparedness of the graduates in the independent management of medical or dental emergencies in the dental office. Surveys conducted in Hong Kong and Manila, reported that a significant proportion of the fresh graduates felt poorly prepared in managing medical emergencies in dental office.[22,23] Such a disconnection could be the reflection of either inadequate training or a change in practice – circumstances demanding more than what the graduates have been trained for, or a combination of both.
In our study, a greater proportion of women perceived themselves to be well prepared than men, while most of the existing research reported greater preparedness among men.[9,23-26] One reason for better overall preparedness among women in our study could be the constitution of our tool, which gave equal weightage to all domains of practice preparedness. Domains of communication and interpersonal skills and patient-centered care had the same weightage as that of general oral health assessment and technical competence in clinical care. However, the better performance among women cannot be solely attributed to this aspect. A greater proportion of women had indeed rated themselves better prepared in two of the items in even a domain like technical competence, which is traditionally considered a strong area of the male graduates. Although the advantage of females in positive preparedness outcomes did not persist in the multivariate analysis, the role of gender in determining the employability of a graduate needs to be explored further through primary research.
The difference in self-rating between the graduates belonging to the SC category and the other caste groups was most apparent in the domains of communication and interpersonal skills and independent management of practice (especially in their ability to independently manage patients). Poor preparedness in these domains need not be solely a function of the training received. The poor socio-economic context, social backwardness, and poor social capital of the students could impact confidence, participation, communication, and integration.[27] In our study, we have not explored the pathways through which caste may have exerted its influence on self-reported preparedness scores.
There have been numerous reports indicating the decline in quality of higher education, especially health and technical education since the commercialization of the sector.[28] There have been concerns raised regarding the regulation of private dental colleges in the country including a Comptroller and Auditor General Report of 2012, which raised the issue of faculty shortages and irregular attendance.[29] This difference in preparedness scores between public and private sector trained graduates necessitate an enquiry into the quality of training in the private sector, which has been a matter of huge scepticism and discussion from the early phases of commercialization of higher education in the country.
CONCLUSION
A significant proportion of our study participants reported lower preparedness for independent practice, reflecting poor self-rating of their employability. When placed in the context of the saturated job market and rising unemployment among young dentists, this is a critical finding. The relatively higher proportion of poor preparedness among the private sector trained graduates when compared to the government college trained graduates is another matter that raises concern. Both these findings necessitate an enquiry into the extent to which the current system of undergraduate training informs the demands of independent practice. Job insecurity reflected as frequent job changes also seems to contribute to poor preparedness. The role played by gender and caste in determining the level of preparedness and the pathways through which these social factors influence the professional readiness of the dental graduates is another area that mandates further research.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Failure of policy initiatives in regulating health professional education: The case of dental education in India. J Health Manag. 2018;20:88-91.
- [CrossRef] [Google Scholar]
- Medical education in India: Is it still possible to reverse the downhill trend. Natl Med J India. 2010;23:156-60.
- [Google Scholar]
- The Economics of Health Professional Education and Careers. In: Insights from a Literature Review. Washington DC: World Bank studies; 2015.
- [CrossRef] [Google Scholar]
- Exponential growth of dental schools in Chile: Effects on academic, economic and workforce issues. Braz Oral Res (São Paulo). 2013;27:471-7.
- [CrossRef] [PubMed] [Google Scholar]
- Dentistry in Brazil: Its history and current trends. J Dent Educ. 2009;73:225-31.
- [CrossRef] [PubMed] [Google Scholar]
- Unemployment and vulnerable financial situation among recent dental graduates of Kerala, India results from a cross-sectional study. J Global Oral Health. 2019;1:1-9.
- [CrossRef] [Google Scholar]
- Conceptual framework explaining “preparedness for practice” of dental graduates: A systematic review. J Dent Educ. 2018;82:1194-202.
- [CrossRef] [PubMed] [Google Scholar]
- Preparedness and practice management skills of graduating dental students entering the workforce. Educ Res Int. 2015;2015:976124.
- [CrossRef] [Google Scholar]
- Online Kappa Calculator. 2017. Available from: http://www.justus.randolphname/kappa [Last accessed on 2018 Apr 4]
- [Google Scholar]
- Do dental graduates of the University of Hong Kong (1997-2001) perceive themselves prepared for dental practice. Hong Kong Dent J. 2005;2:84-91.
- [Google Scholar]
- Undergraduate training as preparation for vocational training in England: A survey of vocational dental practitioners and their trainers' views. Br Dent J. 2006;6(Suppl):9-15.
- [CrossRef] [PubMed] [Google Scholar]
- Self-perceived preparedness for dental practice amongst graduates of the University of Hong Kong's integrated PBL dental curriculum. Eur J Dent Educ. 2012;16:96-105.
- [CrossRef] [PubMed] [Google Scholar]
- Toward a reliable and valid measure of institutional mission and values perception: The DePaul Values Inventory. J Beliefs Values. 2004;25:43-54.
- [CrossRef] [Google Scholar]
- Assessing college students' satisfaction with their academic majors. J Career Assess. 2007;15:446-62.
- [CrossRef] [Google Scholar]
- Involved and focused? Students' perceptions of institutional identity, personal goal orientation and levels of campus engagement. Coll Stud J. 2009;43:886-96.
- [Google Scholar]
- Self-perceived work preparedness of the graduating dental students. Eur J Dent Educ. 2012;17:101-5.
- [CrossRef] [PubMed] [Google Scholar]
- Novice nurses' experiences of unpreparedness at the beginning of the work. Glob J Health Sci. 2014;6:215-22.
- [CrossRef] [PubMed] [Google Scholar]
- Perceptions of the preparedness of medical graduates for internship responsibilities in district hospitals in Kenya: A qualitative study. BMC Med Educ. 2015;15:178.
- [CrossRef] [PubMed] [Google Scholar]
- The experiences of newly graduated nurses during their first year of practice in the Sultanate of Oman a case study. Int J Nurs Stud. 2015;52:1723-34.
- [CrossRef] [PubMed] [Google Scholar]
- Graduates' perceived preparedness for dental practice from PBL and traditional curricula. J Dent Educ. 2011;75:1270-29.
- [CrossRef] [PubMed] [Google Scholar]
- Self-concept and variables related to preparedness for dental practice: Basis for a proposed program enhancement. J Advocacy Res Educ. 2015;2:86-91.
- [Google Scholar]
- Western Australian dental graduates' perception of preparedness to practice: A five-year follow-up. J Dent Educ. 2007;71:1217-22.
- [CrossRef] [PubMed] [Google Scholar]
- The undergraduate preparation of dentists: Confidence levels of final year dental students at the School of Dentistry in Cardiff. Br Dent J. 2016;221:349-54.
- [CrossRef] [PubMed] [Google Scholar]
- Preparedness of undergraduate dental students in the United Kingdom: A national study. Br Dent J. 2017;222:472-7.
- [CrossRef] [PubMed] [Google Scholar]
- How prepared are foundation dentists in England and Wales for independent general dental practice. Br Dent J. 2017;223:359-68.
- [CrossRef] [PubMed] [Google Scholar]
- Survey at an IIT campus shows how caste affects students' perceptions. Econ Polit Wkly. 2018;53(9) Available from: https://www.epw.in/node/151160/pdf [Last accessed on 2018 July 5]
- [Google Scholar]
- Introduction In: Kapur D, Mehta PB, eds. Navigating the Labyrinth: Perspectives on India's Higher Education. Hyderabad: Oriental Blackswan; 2017. p. :3.
- [Google Scholar]
- Report of the Comptroller and Auditor General of India for the year ended March 2011. 2012. Union Government (Civil) Autonomous Bodies Audit Number 14 of 2012-13. :95-143. Available from: https://www.cag.gov.in/content/report-no-14-2012-13-union-government-civil-autonomous-bodies-performance-audit [Last accessed on 2018 Nov 15]
- [Google Scholar]




